Esteve Francisco, Lopez-Delgado Juan C, Javierre Casimiro, Skaltsa Konstantina, Carrio Maria Ll, Rodríguez-Castro David, Torrado Herminia, Farrero Elisabet, Diaz-Prieto Antonio, Ventura Josep Ll, Mañez Rafael
Intensive Care Department, Hospital Universitari de Bellvitge, IDIBELL (Institut d'Investigació Biomèdica Bellvitge; Biomedical Investigation Institute of Bellvitge), L'Hospitalet de Llobregat, C/Feixa Llarga s/n., 08907, Barcelona, Spain.
Physiological Sciences II Department, Universitat de Barcelona, IDIBELL, Barcelona, Spain.
BMC Anesthesiol. 2014 Sep 26;14:83. doi: 10.1186/1471-2253-14-83.
The arterial partial pressure of O2 and the fraction of inspired oxygen (PaO2/FiO2) ratio is widely used in ICUs as an indicator of oxygenation status. Although cardiac surgery and ICU scores can predict mortality, during the first hours after cardiac surgery few instruments are available to assess outcome. The aim of this study was to evaluate the usefulness of PaO2/FIO2 ratio to predict mortality in patients immediately after cardiac surgery.
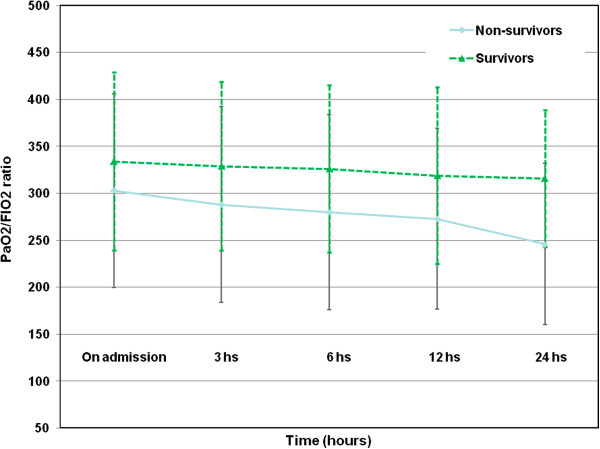
We prospectively studied 2725 consecutive cardiac surgery patients between 2004 and 2009. PaO2/FiO2 ratio was measured on admission and at 3 h, 6 h, 12 h and 24 h after ICU admission, together with clinical data and outcomes.
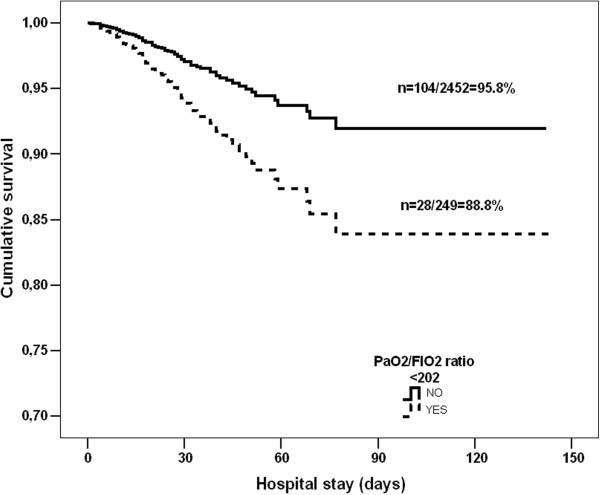
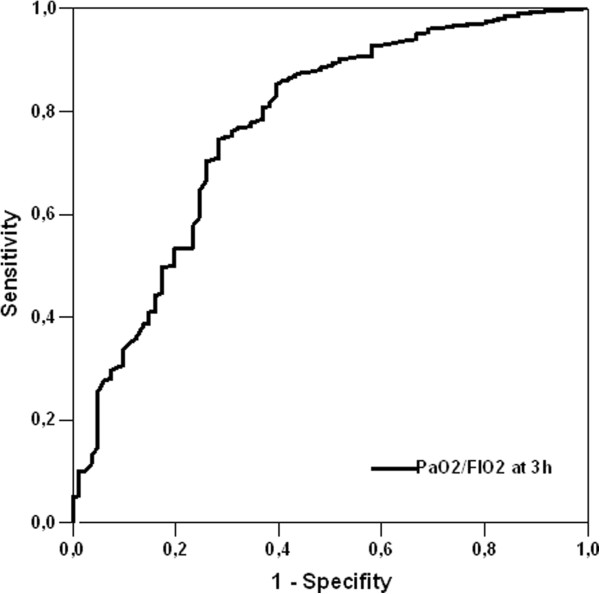
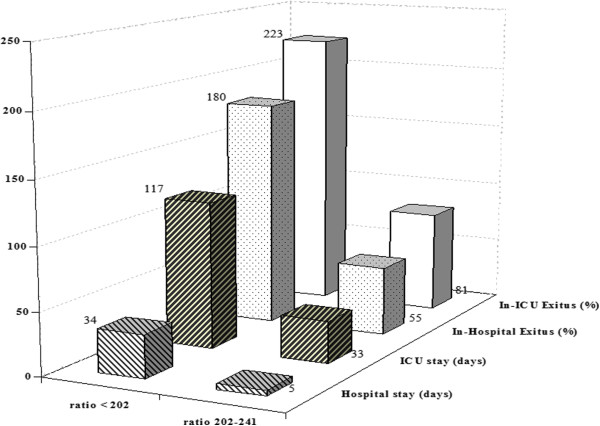
All PaO2/FIO2 ratio measurements differed between survivors and non-survivors (p < 0.001). The PaO2/FIO2 at 3 h after ICU admission was the best predictor of mortality based on area under the curve (p < 0.001) and the optimum threshold estimation gave an optimal cut-off of 222 (95% Confidence interval (CI): 202-242), yielding three groups of patients: Group 1, with PaO2/FIO2 > 242; Group 2, with PaO2/FIO2 from 202 to 242; and Group 3, with PaO2/FIO2 < 202. Group 3 showed higher in-ICU mortality and ICU length of stay and Groups 2 and 3 also showed higher respiratory complication rates. The presence of a PaO2/FIO2 ratio < 202 at 3 h after admission was shown to be a predictor of in-ICU mortality (OR:1.364; 95% CI:1.212-1.625, p < 0.001) and of worse long-term survival (88.8% vs. 95.8%; Log rank p = 0.002. Adjusted Hazard ratio: 1.48; 95% CI:1.293-1.786; p = 0.004).
A simple determination of PaO2/FIO2 at 3 h after ICU admission may be useful to identify patients at risk immediately after cardiac surgery.
动脉血氧分压与吸入氧分数(PaO2/FiO2)比值在重症监护病房(ICU)中被广泛用作氧合状态的指标。虽然心脏手术和ICU评分可以预测死亡率,但在心脏手术后的最初几个小时内,几乎没有可用的工具来评估预后。本研究的目的是评估PaO2/FiO2比值对预测心脏手术后即刻患者死亡率的有用性。
我们对2004年至2009年间连续的2725例心脏手术患者进行了前瞻性研究。在入院时以及入住ICU后3小时、6小时、12小时和24小时测量PaO2/FiO2比值,并收集临床数据和预后情况。
存活者与非存活者的所有PaO2/FiO2比值测量结果均存在差异(p<0.001)。基于曲线下面积,入住ICU后3小时的PaO2/FiO2是死亡率的最佳预测指标(p<0.001),最佳阈值估计得出的最佳截断值为222(95%置信区间(CI):202 - 242),将患者分为三组:第1组,PaO2/FiO2>242;第2组,PaO2/FiO2为202至242;第3组,PaO2/FiO2<202。第3组的ICU死亡率和ICU住院时间更高,第2组和第3组的呼吸并发症发生率也更高。入院后3小时PaO2/FiO2比值<202被证明是ICU死亡率(比值比:1.364;95%CI:1.212 - 1.625,p<0.001)和长期生存较差(88.8%对95.8%;对数秩检验p = 0.002。校正风险比:1.48;95%CI:1.293 - 1.786;p = 0.004)的预测指标。
入住ICU后3小时简单测定PaO2/FiO2可能有助于识别心脏手术后即刻的高危患者。