Department of Thoracic and Cardiovascular Surgery, Nanjing First Hospital, Nanjing Medical University, No. 68 Changle Road, Nanjing, 210006, China.
Department of Biostatistics, School of Public Health, Nanjing Medical University, No. 101 Longmian Avenue, Nanjing, 211166, China.
J Transl Med. 2022 Apr 9;20(1):166. doi: 10.1186/s12967-022-03351-5.
Acute kidney injury (AKI) is a major complication following cardiac surgery that substantially increases morbidity and mortality. Current diagnostic guidelines based on elevated serum creatinine and/or the presence of oliguria potentially delay its diagnosis. We presented a series of models for predicting AKI after cardiac surgery based on electronic health record data.
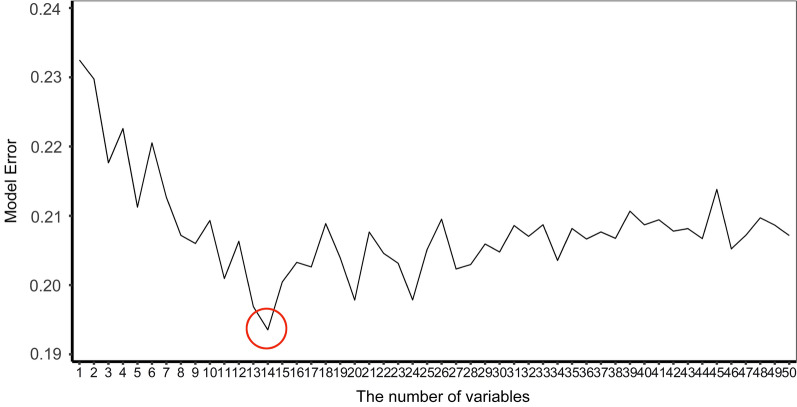
We enrolled 1457 adult patients who underwent cardiac surgery at Nanjing First Hospital from January 2017 to June 2019. 193 clinical features, including demographic characteristics, comorbidities and hospital evaluation, laboratory test, medication, and surgical information, were available for each patient. The number of important variables was determined using the sliding windows sequential forward feature selection technique (SWSFS). The following model development methods were introduced: extreme gradient boosting (XGBoost), random forest (RF), deep forest (DF), and logistic regression. Model performance was accessed using the area under the receiver operating characteristic curve (AUROC). We additionally applied SHapley Additive exPlanation (SHAP) values to explain the RF model. AKI was defined according to Kidney Disease Improving Global Outcomes guidelines.
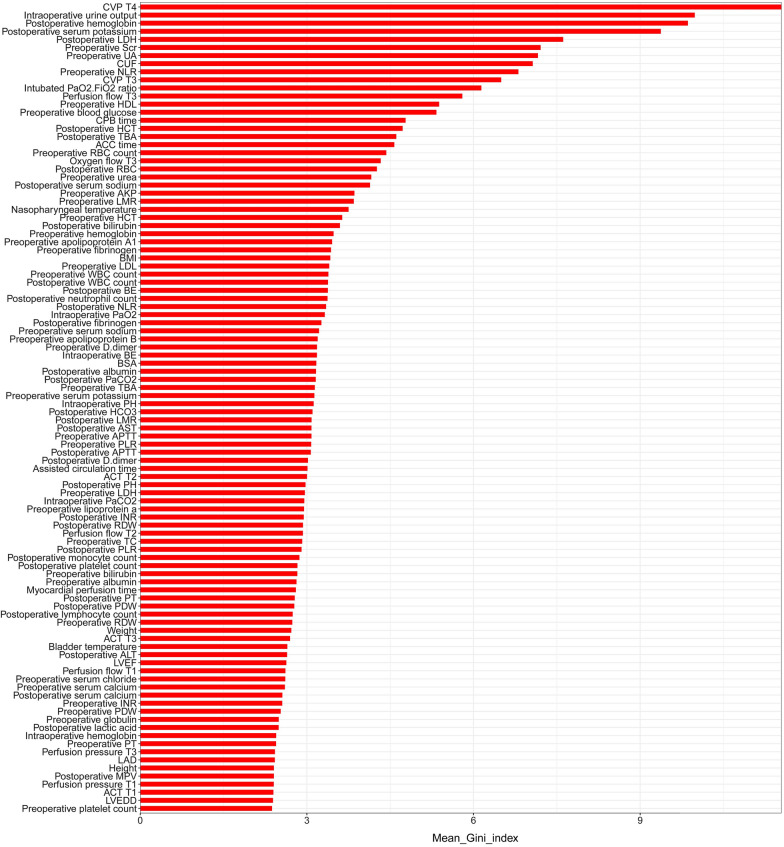
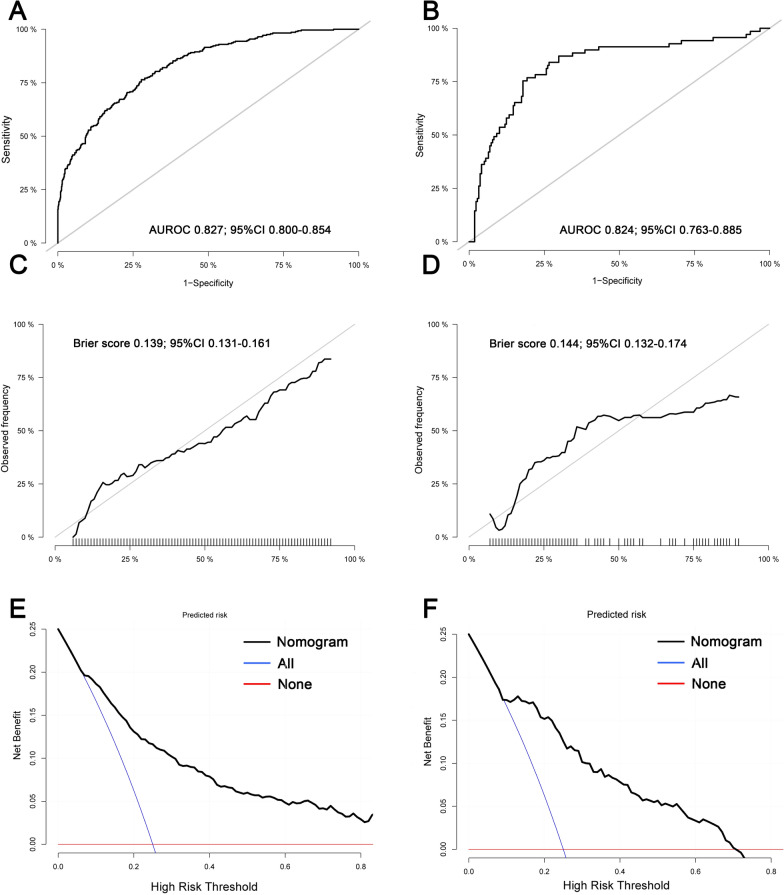
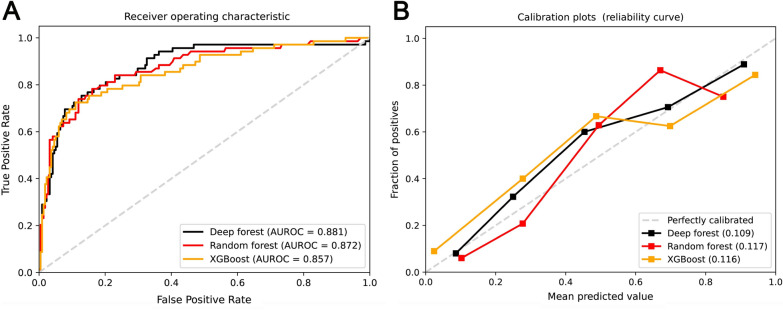
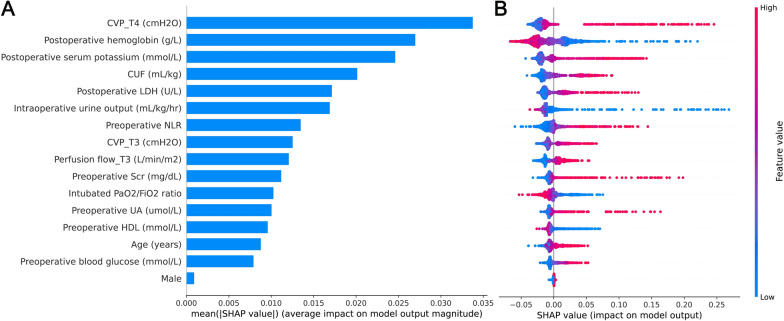
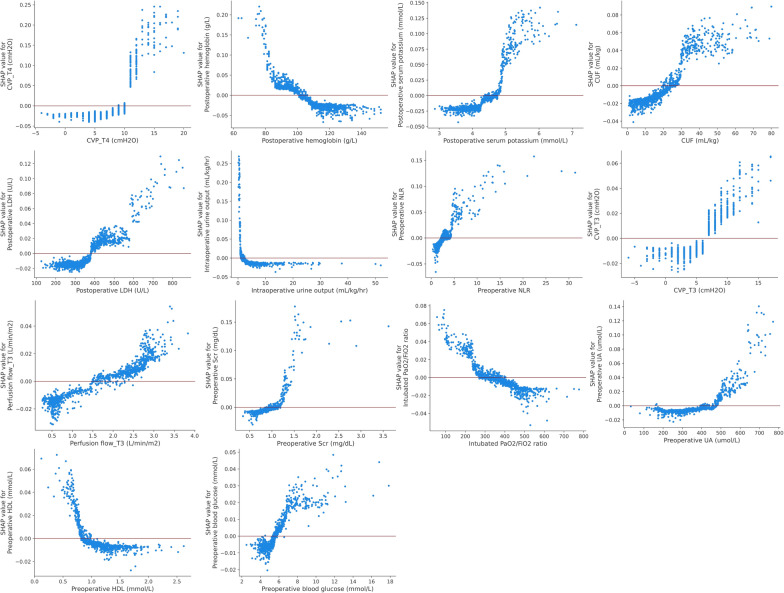
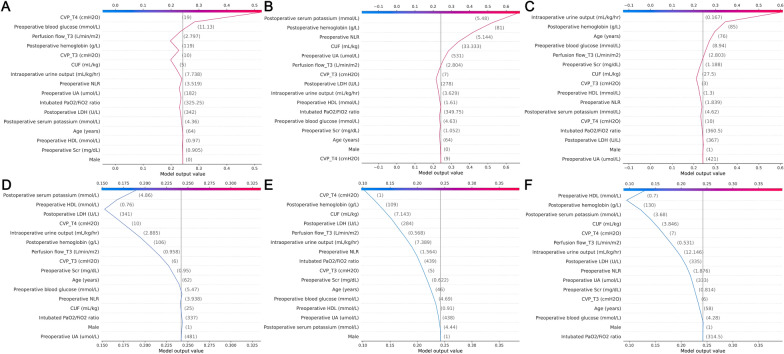
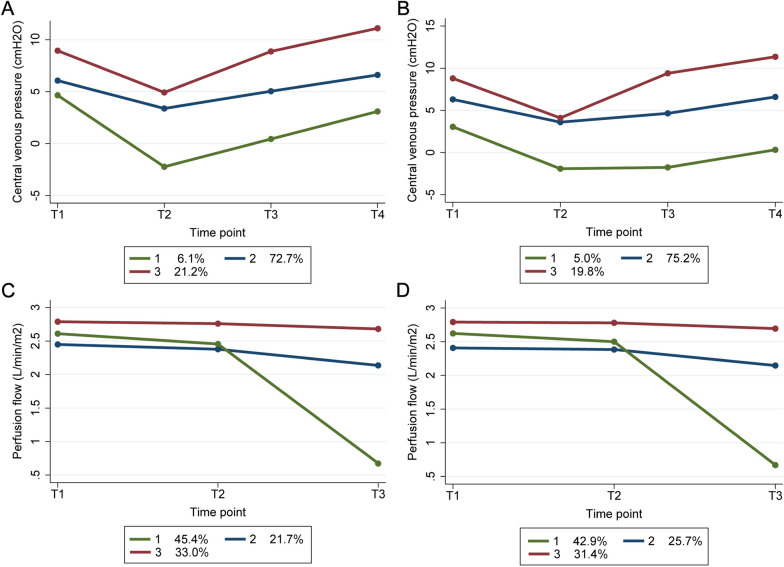
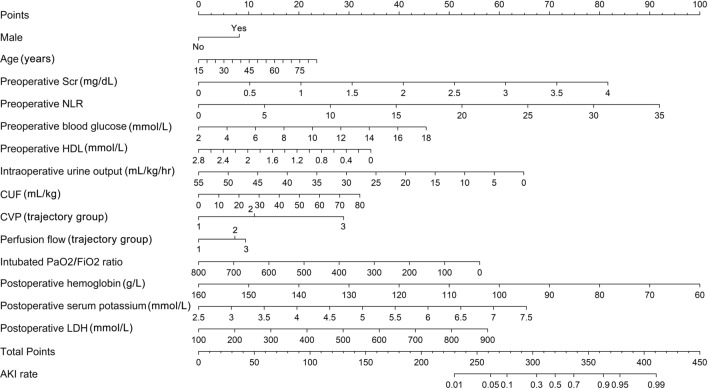
In the discovery set, SWSFS identified 16 important variables. The top 5 variables in the RF importance matrix plot were central venous pressure, intraoperative urine output, hemoglobin, serum potassium, and lactic dehydrogenase. In the validation set, the DF model exhibited the highest AUROC (0.881, 95% confidence interval [CI] 0.831-0.930), followed by RF (0.872, 95% CI 0.820-0.923) and XGBoost (0.857, 95% CI 0.802-0.912). A nomogram model was constructed based on intraoperative longitudinal features, achieving an AUROC of 0.824 (95% CI 0.763-0.885) in the validation set. The SHAP values successfully illustrated the positive or negative contribution of the 16 variables attributed to the output of the RF model and the individual variable's effect on model prediction.
Our study identified 16 important predictors and provided a series of prediction models to enhance risk stratification of AKI after cardiac surgery. These novel predictors might aid in choosing proper preventive and therapeutic strategies in the perioperative management of AKI patients.
急性肾损伤(AKI)是心脏手术后的主要并发症,极大地增加了发病率和死亡率。目前基于血清肌酐升高和/或少尿的诊断标准可能会延迟其诊断。我们提出了一系列基于电子健康记录数据预测心脏手术后 AKI 的模型。
我们纳入了 2017 年 1 月至 2019 年 6 月在南京市第一医院接受心脏手术的 1457 名成年患者。每位患者均有 193 个临床特征,包括人口统计学特征、合并症和医院评估、实验室检查、药物和手术信息。使用滑动窗口序贯前向特征选择技术(SWSFS)确定重要变量的数量。引入了以下模型开发方法:极端梯度提升(XGBoost)、随机森林(RF)、深度森林(DF)和逻辑回归。使用接收器操作特征曲线下面积(AUROC)评估模型性能。我们还应用 SHapley Additive exPlanation(SHAP)值来解释 RF 模型。AKI 根据肾脏病改善全球结果指南定义。
在发现集中,SWSFS 确定了 16 个重要变量。RF 重要性矩阵图中的前 5 个变量为中心静脉压、术中尿量、血红蛋白、血清钾和乳酸脱氢酶。在验证集中,DF 模型的 AUROC 最高(0.881,95%置信区间[CI] 0.831-0.930),其次是 RF(0.872,95% CI 0.820-0.923)和 XGBoost(0.857,95% CI 0.802-0.912)。基于术中纵向特征构建了列线图模型,在验证集中的 AUROC 为 0.824(95% CI 0.763-0.885)。SHAP 值成功地说明了 RF 模型输出的 16 个变量的正或负贡献,以及个别变量对模型预测的影响。
我们的研究确定了 16 个重要预测因子,并提供了一系列预测模型,以提高心脏手术后 AKI 的风险分层。这些新的预测因子可能有助于在 AKI 患者围手术期管理中选择适当的预防和治疗策略。