Gozalo Pedro, Plotzke Michael, Mor Vincent, Miller Susan C, Teno Joan M
From the Center for Gerontology and Healthcare Research and the Department of Health Services, Policy, and Practice, School of Public Health, Brown University (P.G., V.M., S.C.M., J.M.T.), and the Providence Veterans Affairs Medical Center, Health Services Research (V.M.) - all in Providence, RI; and Abt Associates, Cambridge, MA (M.P.).
N Engl J Med. 2015 May 7;372(19):1823-31. doi: 10.1056/NEJMsa1408705.
Nursing home residents' use of hospice has substantially increased. Whether this increase in hospice use reduces end-of-life expenditures is unknown.
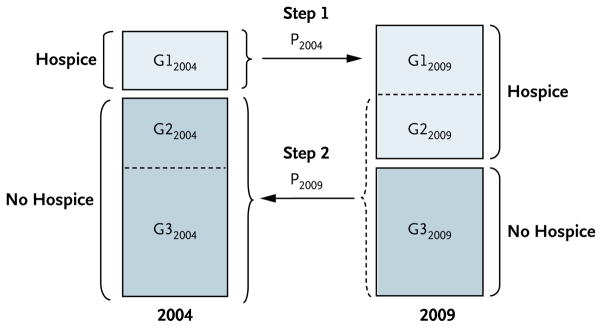
The expansion of hospice between 2004 and 2009 created a natural experiment, allowing us to conduct a difference-in-differences matched analysis to examine changes in Medicare expenditures in the last year of life that were associated with this expansion. We also assessed intensive care unit (ICU) use in the last 30 days of life and, for patients with advanced dementia, feeding-tube use and hospital transfers within the last 90 days of life. We compared a subset of hospice users from 2009, whose use of hospice was attributed to hospice expansion, with a matched subset of non-hospice users from 2004, who were considered likely to have used hospice had they died in 2009.
Of 786,328 nursing home decedents, 27.6% in 2004 and 39.8% in 2009 elected to use hospice. The 2004 and 2009 matched hospice and nonhospice cohorts were similar (mean age, 85 years; 35% male; 25% with cancer). The increase in hospice use was associated with significant decreases in the rates of hospital transfers (2.4 percentage-point reduction), feeding-tube use (1.2 percentage-point reduction), and ICU use (7.1 percentage-point reduction). The mean length of stay in hospice increased from 72.1 days in 2004 to 92.6 days in 2009. Between 2004 and 2009, the expansion of hospice was associated with a mean net increase in Medicare expenditures of $6,761 (95% confidence interval, 6,335 to 7,186), reflecting greater additional spending on hospice care ($10,191) than reduced spending on hospital and other care ($3,430).
The growth in hospice care for nursing home residents was associated with less aggressive care near death but at an overall increase in Medicare expenditures. (Funded by the Centers for Medicare and Medicaid Services and the National Institute on Aging.).
疗养院居民临终关怀服务的使用显著增加。临终关怀服务使用的增加是否能降低临终支出尚不清楚。
2004年至2009年间临终关怀服务的扩张构成了一项自然实验,使我们能够进行双重差分匹配分析,以研究与该扩张相关的临终前一年医疗保险支出的变化。我们还评估了生命最后30天内重症监护病房(ICU)的使用情况,以及患有晚期痴呆症的患者在生命最后90天内鼻饲管的使用情况和医院转诊情况。我们将2009年临终关怀服务使用者的一个子集(其临终关怀服务的使用归因于临终关怀服务的扩张)与2004年非临终关怀服务使用者的一个匹配子集进行了比较,后者如果在2009年去世,被认为很可能会使用临终关怀服务。
在786,328名疗养院死者中,2004年有27.6%,2009年有39.8%选择使用临终关怀服务。2004年和2009年匹配的临终关怀服务使用者和非使用者队列相似(平均年龄85岁;35%为男性;25%患有癌症)。临终关怀服务使用的增加与医院转诊率(降低2.4个百分点)、鼻饲管使用率(降低1.2个百分点)和ICU使用率(降低7.1个百分点)的显著下降相关。临终关怀服务的平均住院时间从2004年的72.1天增加到2009年的92.6天。2004年至2009年间,临终关怀服务的扩张与医疗保险支出平均净增加6,761美元相关(95%置信区间为6,335至7,186美元),这反映出临终关怀服务的额外支出增加(10,191美元),超过了医院和其他护理费用的减少(3,430美元)。
疗养院居民临终关怀服务的增长与临终时积极治疗的减少相关,但医疗保险支出总体增加。(由医疗保险和医疗补助服务中心及国家老龄化研究所资助。)