Čečka Filip, Loveček Martin, Jon Bohumil, Skalický Pavel, Šubrt Zdeněk, Ferko Alexander
Department of Surgery, Faculty of Medicine, University Hospital Hradec Králové, Sokolská 581, 500 05, Hradec Králové, Czech Republic.
First Department of Surgery, Faculty of Medicine, University Hospital Olomouc, IP Pavlova 6, 779 00, Olomouc, Czech Republic.
Trials. 2015 May 7;16:207. doi: 10.1186/s13063-015-0706-1.
The morbidity of pancreatic resection remains high, with pancreatic fistula being the most common cause. The important question is whether any postoperative treatment adjustment may prevent the development of clinically significant postoperative pancreatic fistulae. Recent studies have shown that intraabdominal drains and manipulation using them are of great importance. Although authors of a few retrospective reports have described good results of pancreatic resection without the use of intraabdominal drains, a recent prospective randomized trial showed that routine elimination of drains in pancreaticoduodenectomy is associated with poor outcome. An important issue arises as to which type of drain is most suitable for pancreatic resection. Two types of surgical drains exist: open drains and closed drains. Open drains are considered obsolete nowadays because of frequent retrograde infection. Closed drains include two types: passive gravity drains and closed-suction drains. Closed-suction drains are more effective, as they remove fluid from the abdominal cavity under light pressure. However, some surgeons believe that closed-suction drains represent a potential hazard to patients and that negative pressure might increase the risk of pancreatic fistulae. Nobody has yet specifically dealt with the question of which kind of drainage is most appropriate in pancreatic surgery.
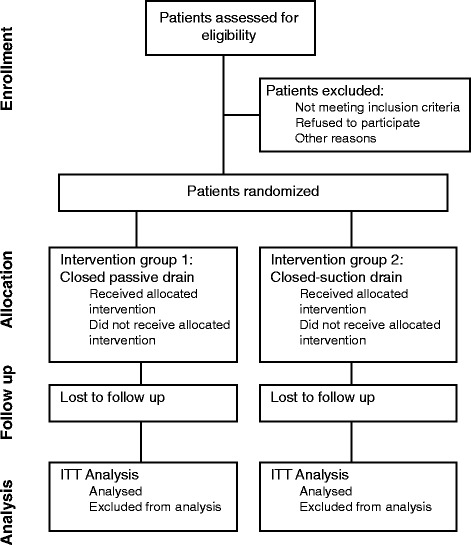
METHODS/DESIGN: The aim of the DRAins in PAncreatic surgery (DRAPA) trial is to compare the closed-suction drain versus the closed passive gravity drain in pancreatic resection. DRAPA is a dual-centre, prospective, randomized controlled trial. The primary endpoint is the rate of postoperative pancreatic fistula; the secondary endpoint is postoperative morbidity with follow-up of 3 months.
No study to date has compared different types of drains in pancreatic surgery. This study is designed to answer the question whether any particular type of drain might lower the rate of postoperative pancreatic fistula or other complications.
ClinicalTrials.gov Identifier: NCT01988519. Registered 13 November 2013.
胰腺切除术的发病率仍然很高,胰瘘是最常见的原因。重要的问题是,术后是否进行任何治疗调整可以预防具有临床意义的术后胰瘘的发生。最近的研究表明,腹腔引流管及其使用操作非常重要。虽然一些回顾性报告的作者描述了不使用腹腔引流管进行胰腺切除术的良好结果,但最近一项前瞻性随机试验表明,在胰十二指肠切除术中常规不放置引流管与不良预后相关。一个重要的问题是哪种类型的引流管最适合胰腺切除术。手术引流管有两种类型:开放引流管和闭合引流管。由于频繁发生逆行感染,开放引流管如今被认为已过时。闭合引流管包括两种类型:被动重力引流管和封闭式负压引流管。封闭式负压引流管更有效,因为它们在轻微压力下从腹腔中吸出液体。然而,一些外科医生认为封闭式负压引流管对患者存在潜在危害,负压可能会增加胰瘘的风险。尚未有人专门探讨在胰腺手术中哪种引流方式最合适的问题。
方法/设计:胰腺手术引流(DRAPA)试验的目的是比较胰腺切除术中封闭式负压引流管与闭合被动重力引流管的效果。DRAPA是一项双中心、前瞻性、随机对照试验。主要终点是术后胰瘘的发生率;次要终点是术后3个月随访时的发病率。
迄今为止,尚无研究比较胰腺手术中不同类型的引流管。本研究旨在回答是否有特定类型的引流管可能降低术后胰瘘或其他并发症发生率的问题。
ClinicalTrials.gov标识符:NCT01988519。于2013年11月13日注册。