Pohl Jürgen, Halphen Marc, Kloess Hans Rudolf, Fischbach Wolfgang
Klinikum Friedrichshain, Berlin, Germany.
Norgine Limited, Harefield, United Kingdom.
PLoS One. 2015 May 7;10(5):e0126067. doi: 10.1371/journal.pone.0126067. eCollection 2015.
Efficacy of two low volume bowel cleansing preparations, polyethylene glycol plus ascorbate (PEG + Asc) and sodium picosulfate/magnesium citrate (NaPic/MgCit), were compared for polyp and adenoma detection rate (PDR and ADR) and overall cleansing ability. Primary endpoint was PDR (the number of patients with ≥ 1 polypoid or flat lesion recorded by the colonoscopist).
Diagnostic, surveillance or screening colonoscopy patients were enrolled into this investigator-blinded, multi-center Phase IV study and randomized 1:1 to receive PEG + Asc (administered the evening before and the morning of colonoscopy, per label) or NaPic/MgCit (administered in the morning and afternoon the day before colonoscopy, per label). The blinded colonoscopist documented any lesion and assessed cleansing quality (Harefield Cleansing Scale).
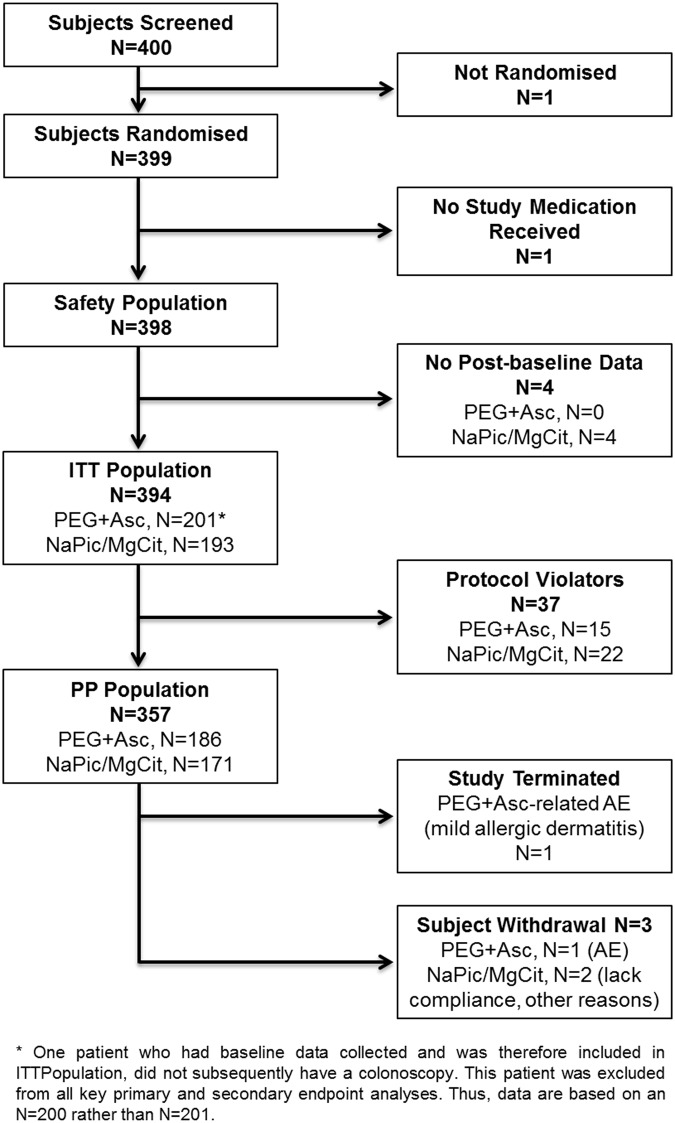
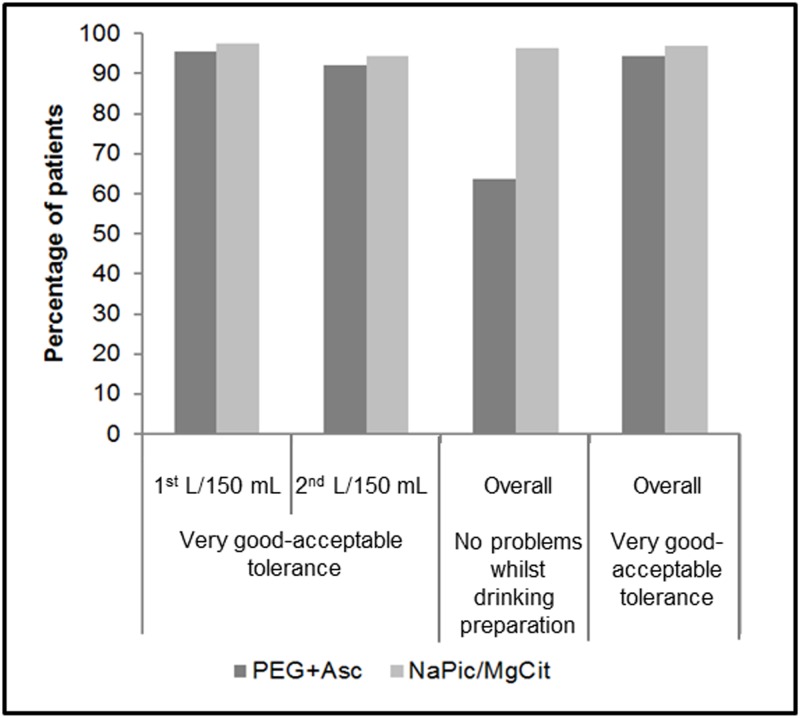
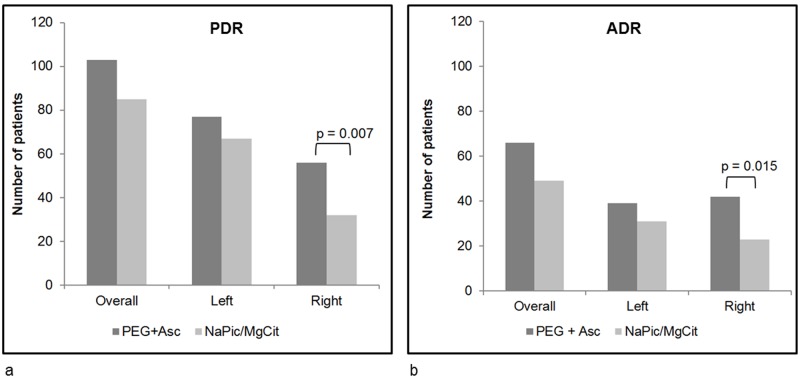
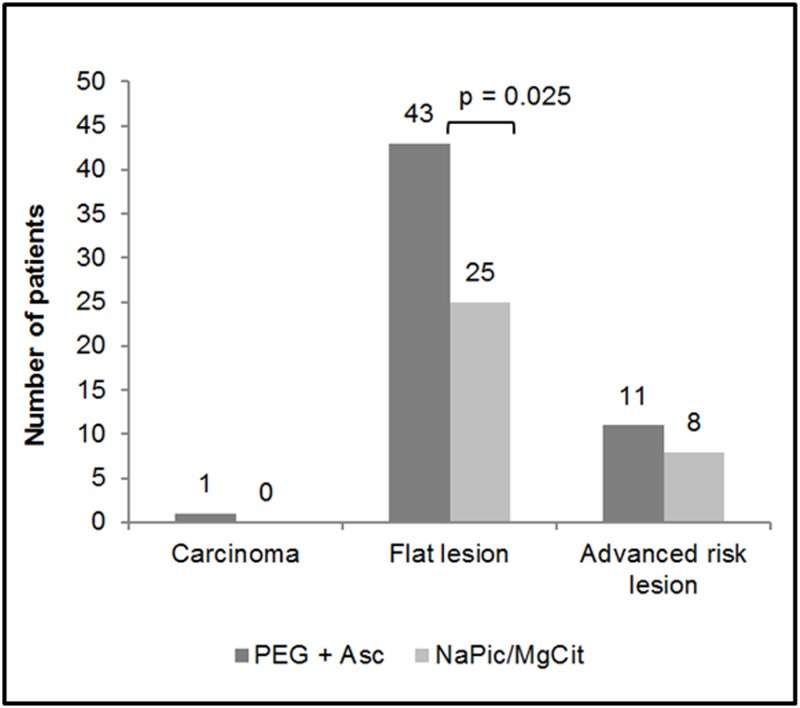
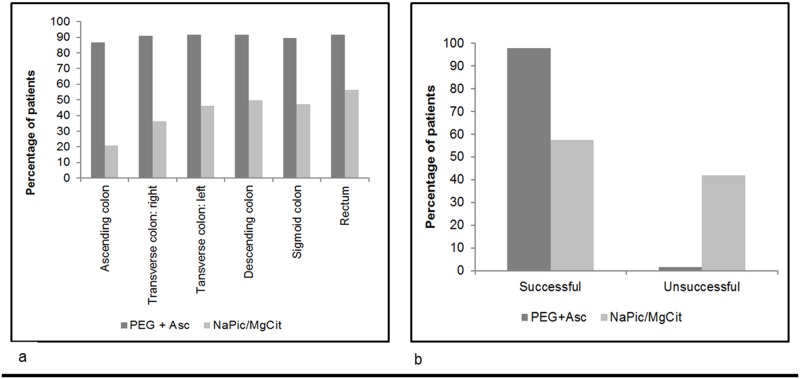
Of 394 patients who completed the study, 393 (PEG + Asc, N = 200; NaPic/MgCit, N = 193) had a colonoscopy. Overall PDR for PEG+Asc versus NaPic/MgCit was 51.5% versus 44.0%, p = 0.139. PDR and ADR on the right side of the bowel were significantly higher with PEG + Asc versus NaPic/MgCit (PDR: 56[28.0%] versus 32[16.6%], p = 0.007; ADR: 42[21.0%] versus 23[11.9%], p = 0.015), as was detection of flat lesions (43[21.5%] versus 25[13.0%], p = 0.025). Cleansing quality was better with PEG + Asc than NaPic/MgCit (98.5% versus 57.5% considered successful cleansing). Overall, there were 132 treatment-emergent adverse events (93 versus 39 for PEG+Asc and NaPic/MgCit, respectively). These were mainly mild abdominal symptoms, all of which were reported for higher proportions of patients in the PEG+Asc than NaPic/MgCit group. Twice as many patients in the NaPic/MgCit versus the PEG + Asc group reported tolerance of cleansing solution as 'very good'.
Compared with NaPic/MgCit, PEG + Asc may be more efficacious for overall cleansing ability, and subsequent detection of right-sided and flat lesions. This is likely attributable to the different administration schedules of the two bowel cleansing preparations, which may positively impact the detection and prevention of colorectal cancer, thereby improving mortality rates.
ClinicalTrials.gov NCT01689792.
比较两种小容量肠道清洁制剂聚乙二醇加抗坏血酸盐(PEG + Asc)和匹可硫酸钠/柠檬酸镁(NaPic/MgCit)在息肉和腺瘤检出率(PDR和ADR)以及整体清洁能力方面的效果。主要终点是PDR(结肠镜检查医师记录的有≥1个息肉样或扁平病变的患者数量)。
将诊断性、监测性或筛查性结肠镜检查患者纳入这项研究者设盲的多中心IV期研究,并按1:1随机分组,分别接受PEG + Asc(按照标签说明,在结肠镜检查前一晚和当天早晨服用)或NaPic/MgCit(按照标签说明,在结肠镜检查前一天的上午和下午服用)。设盲的结肠镜检查医师记录任何病变并评估清洁质量(哈菲尔德清洁量表)。
在完成研究的394例患者中,393例(PEG + Asc组200例;NaPic/MgCit组193例)接受了结肠镜检查。PEG+Asc组与NaPic/MgCit组的总体PDR分别为51.5%和44.0%,p = 0.139。与NaPic/MgCit相比,PEG + Asc组在肠道右侧的PDR和ADR显著更高(PDR:56例[28.0%]对32例[16.6%],p = 0.007;ADR:42例[21.0%]对23例[11.9%],p = 0.015),扁平病变的检出率也是如此(43例[21.5%]对25例[13.0%],p = 0.025)。PEG + Asc的清洁质量优于NaPic/MgCit(98.5%对5�.5%被认为清洁成功)。总体而言,有132例治疗中出现的不良事件(PEG+Asc组93例,NaPic/MgCit组39例)。这些主要是轻度腹部症状,PEG+Asc组中报告这些症状的患者比例均高于NaPic/MgCit组。报告清洁溶液耐受性为“非常好”的NaPic/MgCit组患者数量是PEG + Asc组的两倍。
与NaPic/MgCit相比,PEG + Asc在整体清洁能力以及随后对右侧和扁平病变的检测方面可能更有效。这可能归因于两种肠道清洁制剂不同的给药方案,这可能对结直肠癌的检测和预防产生积极影响,从而提高死亡率。
ClinicalTrials.gov NCT01689792。