Luebke Thomas, Brunkwall Jan
Department of Vascular and Endovascular Surgery, University Hospital of Cologne, Kerpener Str. 62, 50937, Cologne, Germay.
BMC Cardiovasc Disord. 2015 May 9;15:32. doi: 10.1186/s12872-015-0029-x.
Subgroup analyses from randomized controlled trials (RCT) of carotid endarterectomy (CEA) for both symptomatic and asymptomatic carotid stenosis suggest less benefit in women compared to men, due partly to higher age-independent peri-operative risk. However, a meta-analysis of case series and databases focussing on CEA-related gender differences has never been investigated.
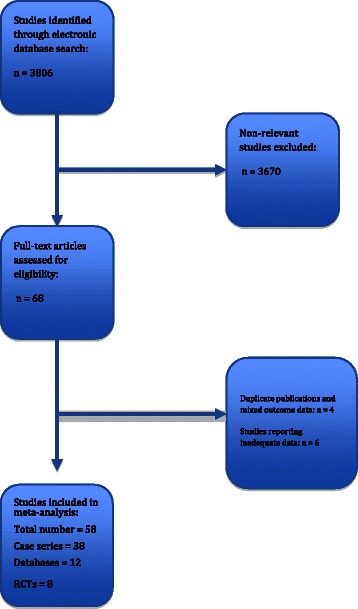
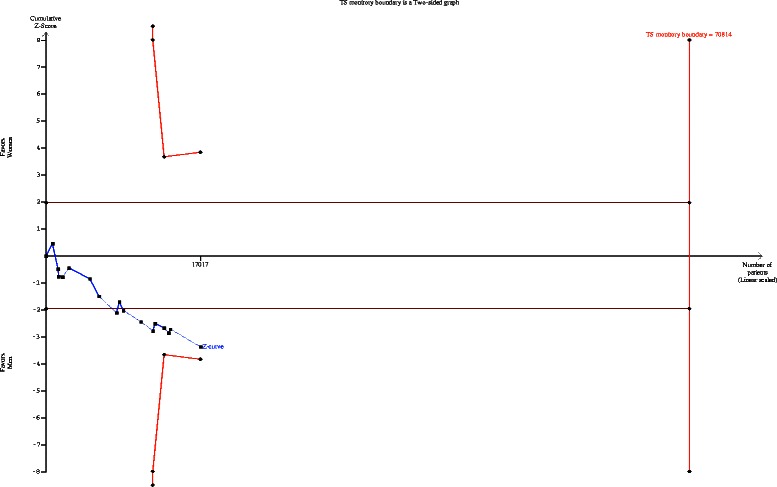
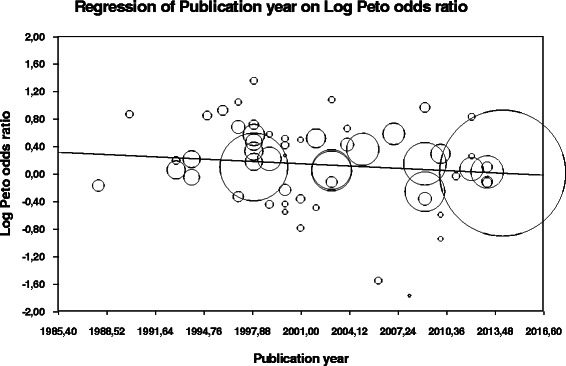
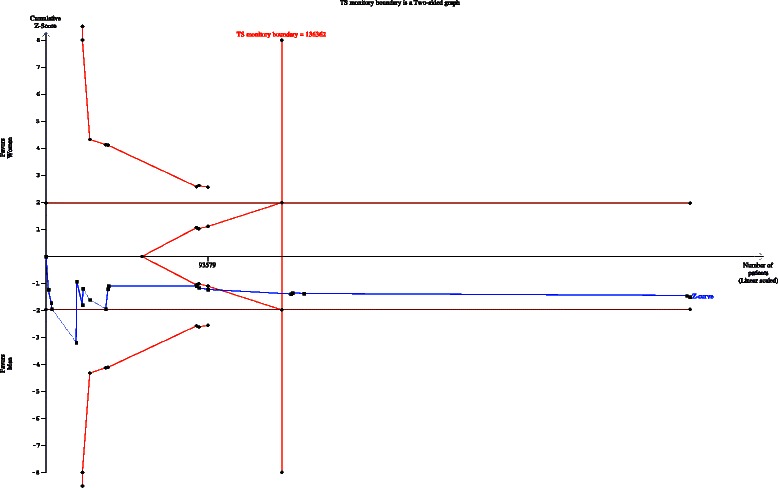
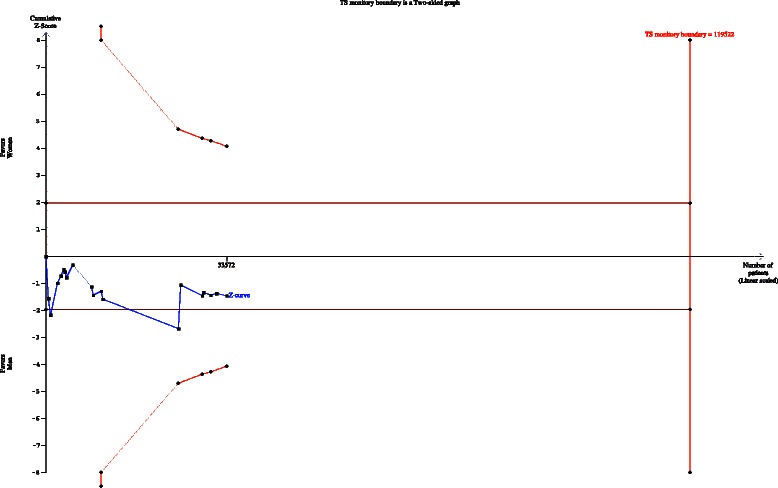
A systematic review of all available publications (including case series, databases and RCTs) reporting data on the association between sex and procedural risk of stroke and/or death following CEA from 1980 to 2015 was investigated. Pooled Peto odds ratios of the procedural risk of stroke and/or death were obtained by Mantel-Haenszel random-effects meta-analysis. The I(2) statistic was used as a measure of heterogeneity. Potential publication bias was assessed with the Egger test and represented graphically with Begg funnel plots of the natural log of the OR versus its standard error. Additional sensitivity analyses were undertaken to evaluate the potential effect of key assumptions and study-level factors on the overall results. Meta-regression models were formed to explore potential heterogeneity as a result of potential risk factors or confounders on outcomes. A tria sequential analysis (TSA) was performed with the aim to maintain an over- all 5% risk of type I error, being the standard in most meta- analyses and systematic reviews.
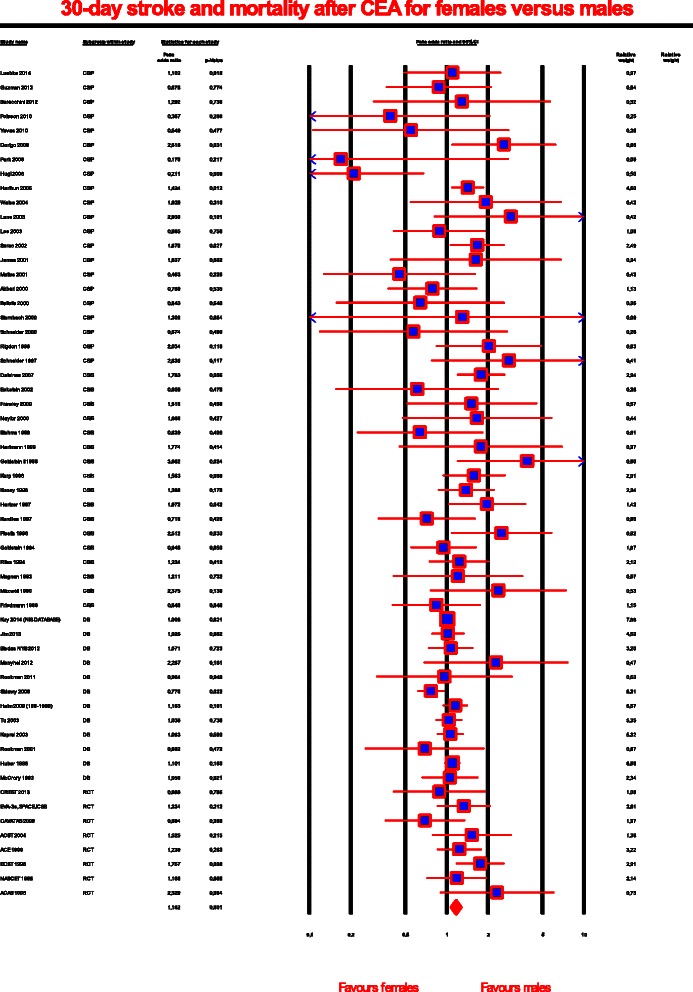
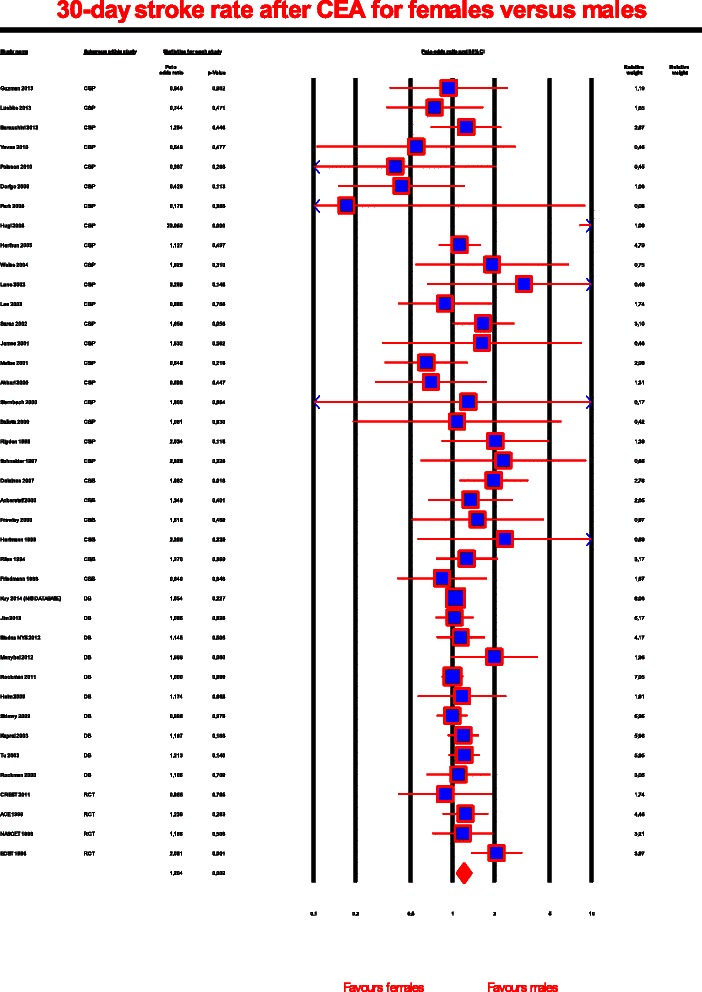
58 articles reported combined stroke and mortality rates within 30 days of treatment. In the unselected overall meta-analysis, the incidence of stroke and death in the male and female groups differed significantly (Peto OR, 1,162; 95% CI, 1.067-1.266; P = .001), revealing a worse outcome for female patients. Moderate heterogeneity among the studies was identified (I(2) = 36%), and the possibility of publication bias was low (P = .03). In sensitivity analyses the meta-analysis of case series with gender aspects as a secondary outcome showed a significantly increased risk for 30-day stroke and death in women compared to men (Peto OR, 1.390; 95% CI, 1.148-1.684; P = .001), In contrast, meta-analysis of databases (Peto OR, 1.025; 95% CI, 0.958-1.097; P = .474) and case series with gender related outcomes as a primary aim (Peto OR, 1.202; 95% CI, 0.925-1.561; P = .168) demonstrated no increase in operative risk of stroke and death in women compared to men.
Meta-analyses of case series and databases dealing with CEA reveal inconsistent results regarding gender differences related to CEA-procedure and should not be transferred into clinical practice.
针对有症状和无症状颈动脉狭窄的颈动脉内膜切除术(CEA)随机对照试验(RCT)的亚组分析表明,与男性相比,女性受益较少,部分原因是与年龄无关的围手术期风险较高。然而,从未对聚焦于CEA相关性别差异的病例系列和数据库进行过荟萃分析。
对1980年至2015年期间所有报告CEA后性别与中风和/或死亡手术风险之间关联数据的可用出版物(包括病例系列、数据库和RCT)进行系统评价。通过Mantel-Haenszel随机效应荟萃分析获得中风和/或死亡手术风险的合并Peto比值比。I(2)统计量用作异质性的度量。用Egger检验评估潜在的发表偏倚,并用OR的自然对数与其标准误的Begg漏斗图以图形方式表示。进行了额外的敏感性分析,以评估关键假设和研究水平因素对总体结果的潜在影响。构建荟萃回归模型,以探讨潜在风险因素或混杂因素对结局造成潜在异质性的情况。进行了序贯分析(TSA),目的是将I型错误的总体风险维持在5%,这是大多数荟萃分析和系统评价的标准。
58篇文章报告了治疗后30天内的中风和死亡率。在未选择的总体荟萃分析中,男性和女性组的中风和死亡发生率有显著差异(Peto比值比,1.162;95%置信区间,1.067 - 1.266;P = 0.001),表明女性患者的结局更差。研究中发现存在中度异质性(I(2)= 36%),发表偏倚的可能性较低(P = 0.03)。在敏感性分析中,将性别因素作为次要结局的病例系列荟萃分析显示,女性30天中风和死亡风险相比男性显著增加(Peto比值比,1.390;95%置信区间,1.148 - 1.684;P = 0.001)。相比之下,数据库的荟萃分析(Peto比值比,1.025;95%置信区间,0.958 - 1.097;P = 0.474)以及将性别相关结局作为主要目的的病例系列荟萃分析(Peto比值比,1.202;95%置信区间,0.925 - 1.561;P = 0.168)表明,女性与男性相比,中风和死亡的手术风险没有增加。
关于CEA的病例系列和数据库的荟萃分析揭示了与CEA手术相关的性别差异的不一致结果,不应将其应用于临床实践。