Jeong Jeong-Won, Lee Jessica, Kamson David O, Chugani Harry T, Juhász Csaba
Translational Imaging Laboratory, Children's Hospital of Michigan, Detroit, MI, USA; Carman and Ann Adams Department of Pediatrics, School of Medicine, Wayne State University, Detroit, MI, USA; Department of Neurology, School of Medicine, Wayne State University, Detroit, MI, USA.
School of Medicine, Wayne State University, Detroit, MI, USA.
Magn Reson Imaging. 2015 Sep;33(7):895-902. doi: 10.1016/j.mri.2015.05.003. Epub 2015 May 7.
To examine whether an objective segmenation of corticospinal tract (CST) associated with hand and leg movements can be used to detect central motor weakness in the corresponding extremities in a pediatric population.
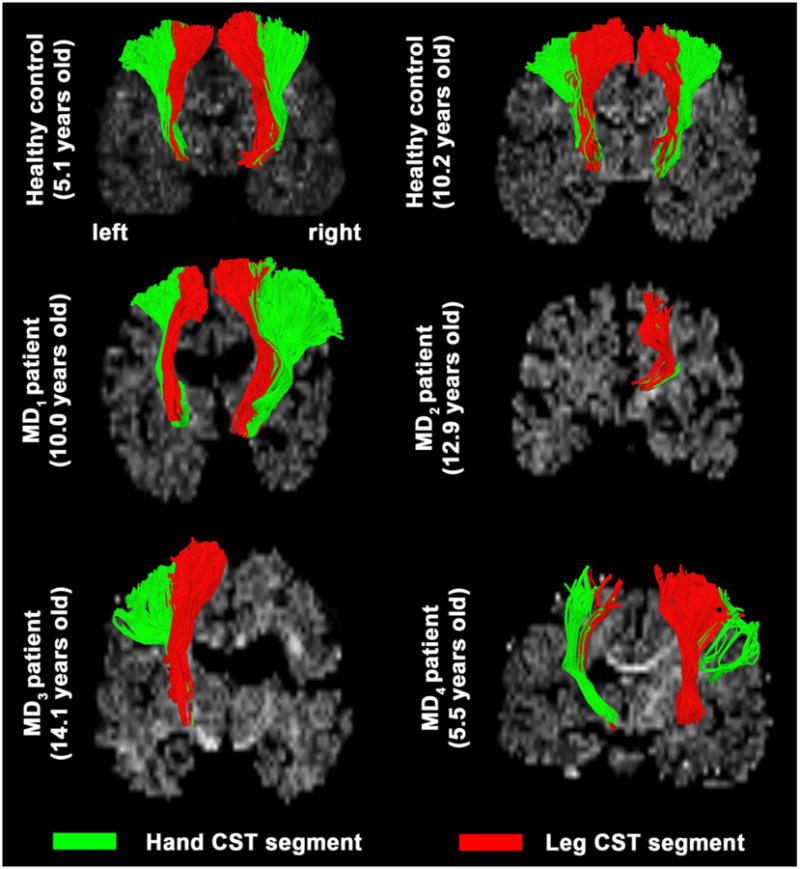
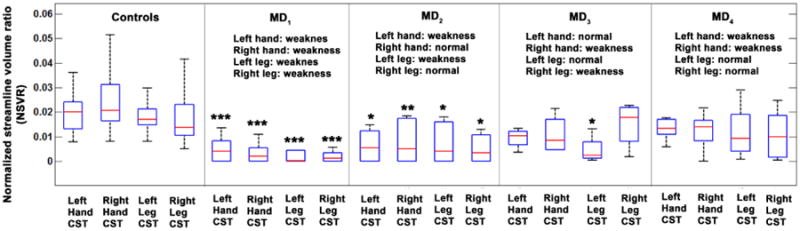
This retrospective study included diffusion tensor imaging (DTI) of 25 children with central paresis affecting at least one limb (age: 9.0±4.2years, 15 boys, 5/13/7 children with left/right/both hemispheric lesions including ischemia, cyst, and gliosis), as well as 42 pediatric control subjects with no motor dysfunction (age: 9.0±5.5years, 21 boys, 31 healthy/11 non-lesional epilepsy children). Leg- and hand-related CST pathways were segmented using DTI-maximum a posteriori (DTI-MAP) classification. The resulting CST volumes were then divided by total supratentorial white matter volume, resulting in a marker called "normalized streamline volume ratio (NSVR)" to quantify the degree of axonal loss in separate CST pathways associated with leg and hand motor functions. A receiver operating characteristic curve was applied to measure the accuracy of this marker to identify extremities with motor weakness.
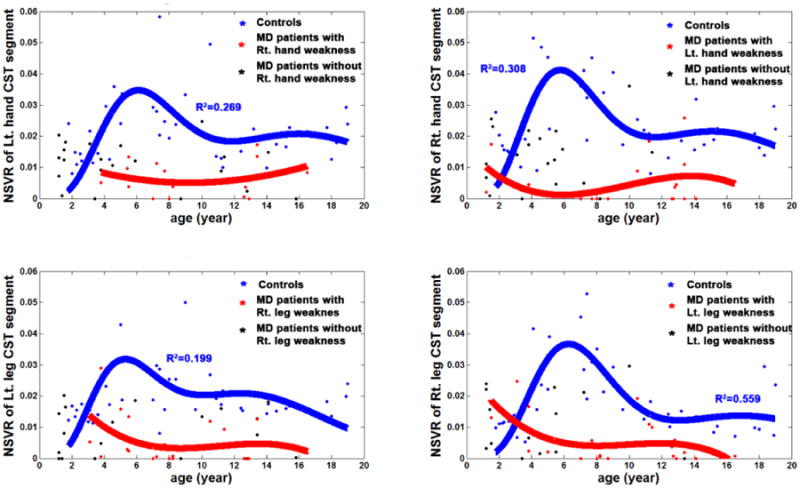
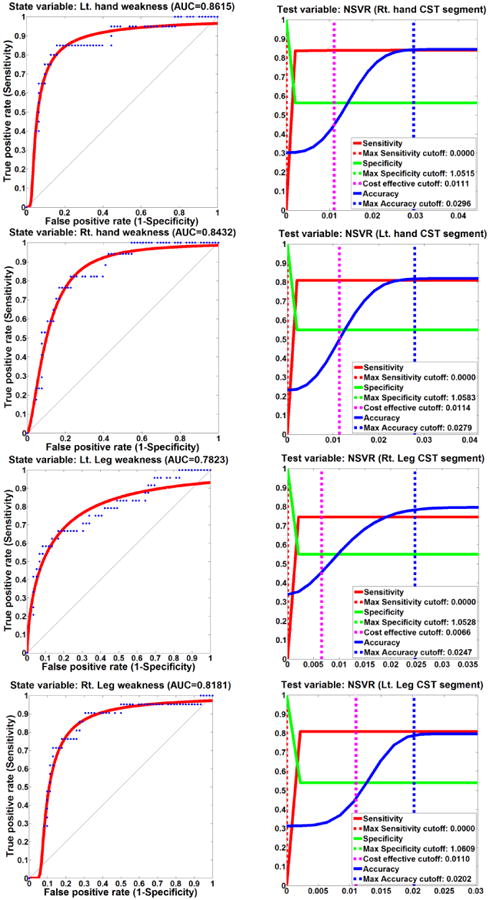
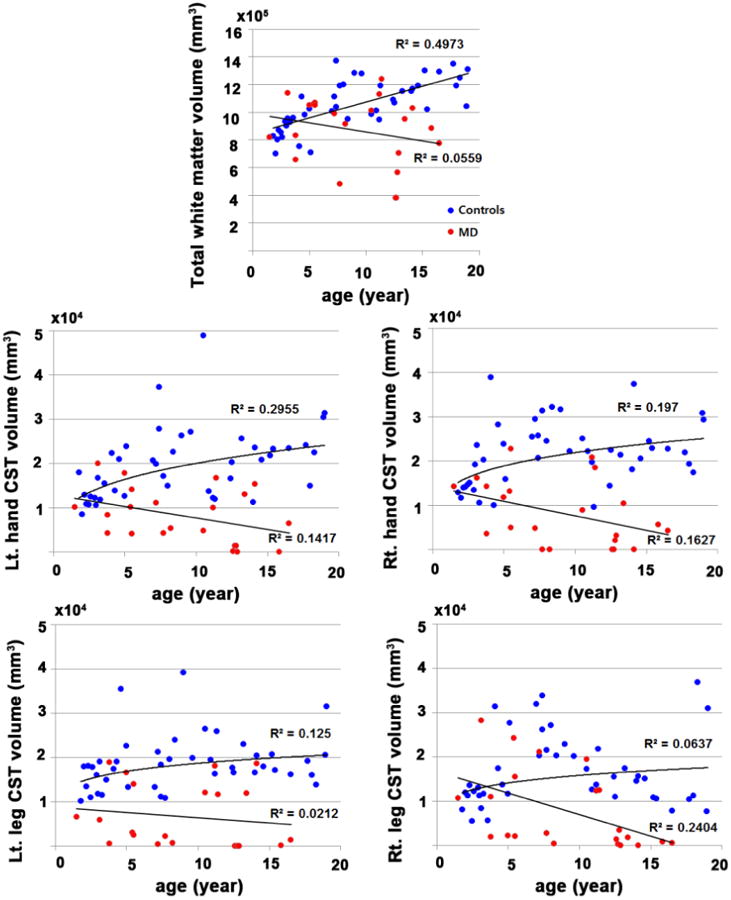
NSVR values of hand/leg CST selectively achieved the following values of accuracy/sensitivity/specificity: 0.84/0.84/0.57, 0.82/0.81/0.55, 0.78/0.75/0.55, 0.79/0.81/0.54 at a cut-off of 0.03/0.03/0.03/0.02 for right hand CST, left hand CST, right leg CST, and left leg CST, respectively. Motor weakness of hand and leg was most likely present at the cut-off values of hand and leg NSVR (i.e., 0.029/0.028/0.025/0.020 for left-hand/right-hand/left-leg/right-leg). The control group showed a moderate age-related increase in absolute CST volumes and a biphasic age-related variation of the normalized CST volumes, which were lacking in the paretic children.
This study demonstrates that DTI-MAP classification may provide a new imaging tool to quantify axonal loss in children with central motor dysfunction. Using this technique, we found that early-life brain lesions affect the maturational trajectory of the primary motor pathway which may be used as an effective marker to facilitate evidence-based treatment of paretic children.
研究与手部和腿部运动相关的皮质脊髓束(CST)的客观分割是否可用于检测儿科人群中相应肢体的中枢运动功能减弱。
这项回顾性研究纳入了25例至少有一个肢体出现中枢性麻痹的儿童的扩散张量成像(DTI)(年龄:9.0±4.2岁,15名男孩,5/13/7例分别患有左/右/双侧半球病变,包括缺血、囊肿和胶质增生),以及42例无运动功能障碍的儿科对照受试者(年龄:9.0±5.5岁,21名男孩,31名健康儿童/11名非病变性癫痫儿童)。使用DTI最大后验概率(DTI-MAP)分类法分割与腿部和手部相关的CST通路。然后将得到的CST体积除以幕上白质总体积,得出一个名为“标准化流线体积比(NSVR)”的指标,以量化与腿部和手部运动功能相关的不同CST通路中的轴突损失程度。应用受试者工作特征曲线来测量该指标识别运动功能减弱肢体的准确性。
手部/腿部CST的NSVR值在右手中枢运动束、左手中枢运动束、右下肢中枢运动束和左下肢中枢运动束的截断值分别为0.03/0.03/0.03/0.02时,选择性地达到了以下准确性/敏感性/特异性值:0.84/0.84/0.57、0.82/0.81/0.55、0.78/0.75/0.55、0.79/0.81/0.54。手部和腿部的运动功能减弱最可能出现在手部和腿部NSVR的截断值处(即左手/右手/左腿/右腿分别为0.029/0.028/0.025/0.020)。对照组显示出绝对CST体积随年龄有适度增加,标准化CST体积随年龄呈双相变化,而麻痹儿童则没有这种变化。
本研究表明,DTI-MAP分类法可能为量化中枢运动功能障碍儿童的轴突损失提供一种新的成像工具。使用该技术,我们发现早期脑损伤会影响主要运动通路的成熟轨迹,这可作为促进对麻痹儿童进行循证治疗的有效指标。