Bradley Steven M, Chan Paul S, Hartigan Pamela M, Nallamothu Brahmajee K, Weintraub William S, Sedlis Steven P, Dada Marcin, Maron David J, Kostuk William J, Berman Daniel S, Teo Koon K, Mancini G B John, Boden William E, Spertus John A
Division of Cardiology, Department of Medicine, VA Eastern Colorado Health Care System, Denver, Colorado; Department of Medicine, University of Colorado School of Medicine at the Anschutz Medical Campus, Aurora, Colorado.
Department of Cardiovascular Research, Saint Luke's Mid America Heart Institute, Missouri; Department of Medicine, University of Missouri-Kansas City, Missouri.
Am J Cardiol. 2015 Jul 15;116(2):167-73. doi: 10.1016/j.amjcard.2015.03.057. Epub 2015 Apr 17.
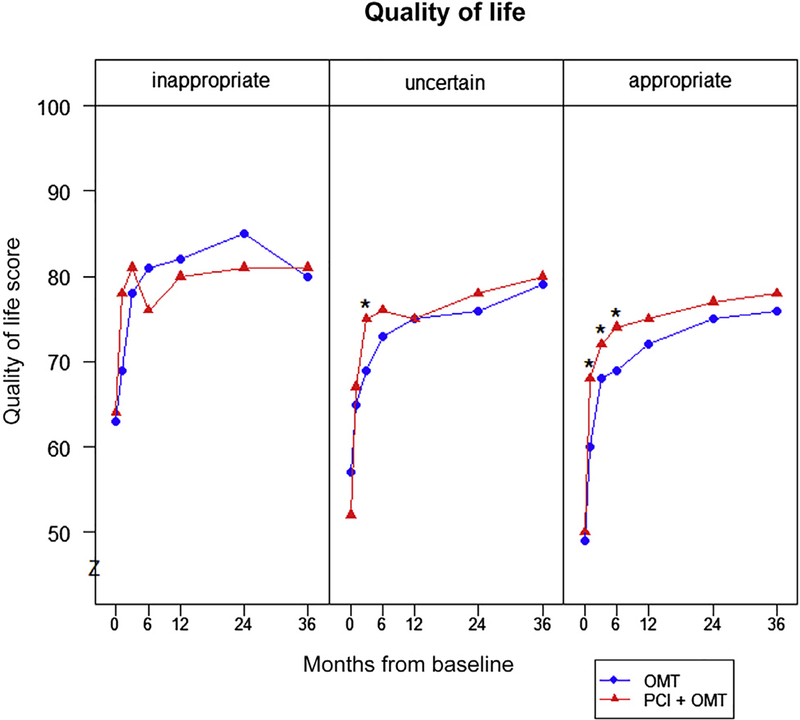
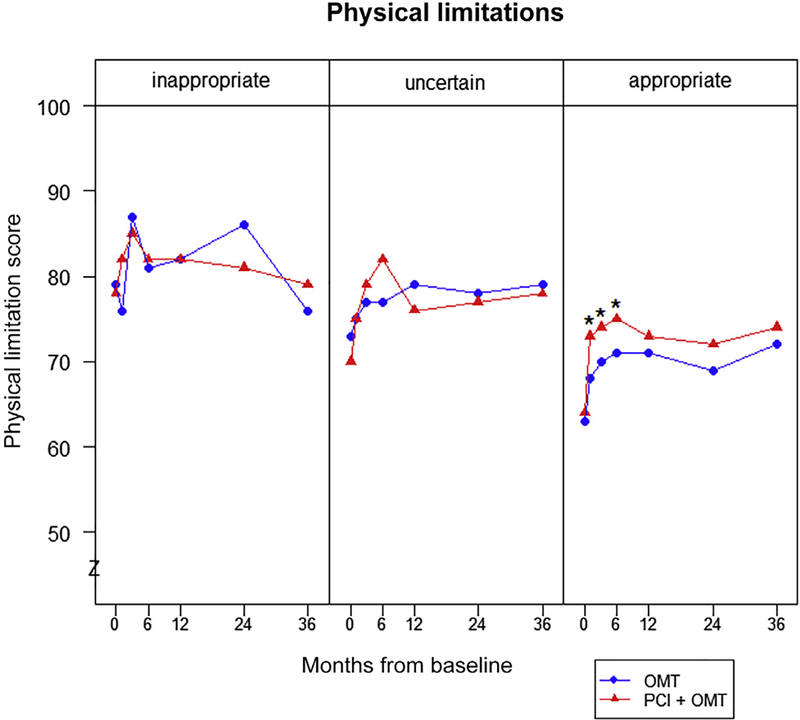
Establishing the validity of appropriate use criteria (AUC) for percutaneous coronary intervention (PCI) in the setting of stable ischemic heart disease can support their adoption for quality improvement. We conducted a post hoc analysis of 2,287 Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation trial patients with stable ischemic heart disease randomized to PCI with optimal medical therapy (OMT) or OMT alone. Within appropriateness categories, we compared rates of death, myocardial infarction, revascularization subsequent to initial therapy, and angina-specific health status as determined by the Seattle Angina Questionnaire in patients randomized to PCI + OMT to those randomized to OMT alone. A total of 1,987 patients (87.9%) were mapped to the 2012 publication of the AUC, with 1,334 (67.1%) classified as appropriate, 551 (27.7%) uncertain, and 102 (5.1%) as inappropriate. There were no significant differences between PCI and OMT alone in the rate of mortality and myocardial infarction by appropriateness classification. Rates of revascularization were significantly lower in patients initially receiving PCI + OMT who were classified as appropriate (hazard ratio 0.65; 95% confidence interval 0.53 to 0.80; p <0.001) or uncertain (hazard ratio 0.49; 95% confidence interval 0.32 to 0.76; p = 0.001). Furthermore, among patients classified as appropriate by the AUC, Seattle Angina Questionnaire scores at 1 month were better in the PCI-treated group compared with the medical therapy group (80 ± 23 vs 75 ± 24 for angina frequency, 73 ± 24 vs 68 ± 24 for physical limitations, and 68 ± 23 vs 60 ± 24 for quality of life; all p <0.01), with differences generally persisting through 12 months. In contrast, health status scores were similar throughout the first year of follow-up in PCI + OMT patients compared with OMT alone in patients classified as uncertain or inappropriate. In conclusion, these findings support the validity of the AUC in efforts to improve health care quality through optimal use of PCI.
确立稳定型缺血性心脏病患者经皮冠状动脉介入治疗(PCI)的合理使用标准(AUC)的有效性,有助于将其应用于质量改进。我们对2287例参加“利用血运重建和强化药物评估进行临床结果研究”试验的稳定型缺血性心脏病患者进行了事后分析,这些患者被随机分为接受PCI联合最佳药物治疗(OMT)组或单纯OMT组。在合适性类别中,我们比较了随机分为PCI + OMT组和单纯OMT组患者的死亡率、心肌梗死发生率、初始治疗后的血运重建率以及由西雅图心绞痛问卷确定的心绞痛特异性健康状况。共有1987例患者(87.9%)被纳入2012年发布的AUC,其中1334例(67.1%)被分类为合适,551例(27.7%)不确定,102例(5.1%)不合适。根据合适性分类,PCI组和单纯OMT组在死亡率和心肌梗死发生率方面无显著差异。初始接受PCI + OMT且被分类为合适(风险比0.65;95%置信区间0.53至0.80;p <0.001)或不确定(风险比0.49;95%置信区间0.32至0.76;p = 0.001)的患者,血运重建率显著较低。此外,在被AUC分类为合适的患者中,PCI治疗组1个月时的西雅图心绞痛问卷评分优于药物治疗组(心绞痛频率:80±23 vs 75±24,身体限制:73±24 vs 68±24,生活质量:68±23 vs 60±24;均p <0.01),这些差异通常持续到12个月。相比之下,在被分类为不确定或不合适的患者中,PCI + OMT组患者在随访的第一年中健康状况评分与单纯OMT组相似。总之,这些发现支持了AUC在通过优化PCI使用来提高医疗质量方面的有效性。