Padala Santosh K, Sidhu Mandeep S, Hartigan Pamela M, Maron David J, Teo Koon K, Spertus John A, Mancini G B John, Sedlis Steven P, Chaitman Bernard R, Heller Gary V, Weintraub William S, Boden William E
Department of Medicine, Albany Medical Center, Albany, New York.
Department of Medicine, Albany Medical Center, Albany, New York; Department of Medicine, Samuel S. Stratton VA Medical Center and Albany Medical College, Albany, New York.
Am J Cardiol. 2015 Nov 15;116(10):1509-15. doi: 10.1016/j.amjcard.2015.08.012. Epub 2015 Aug 31.
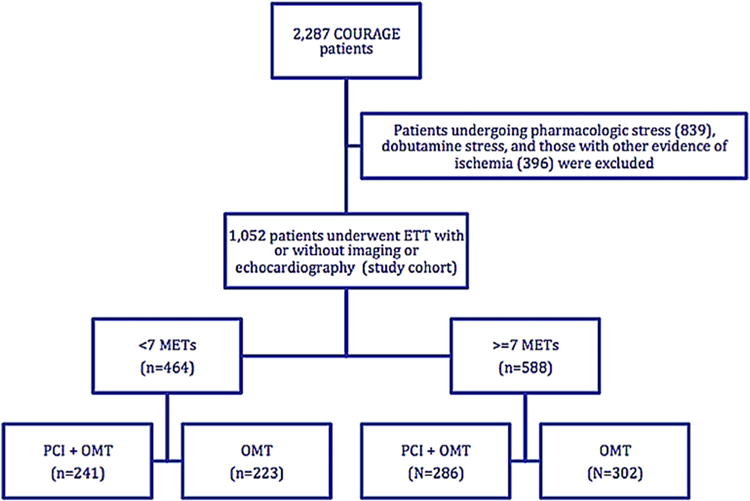
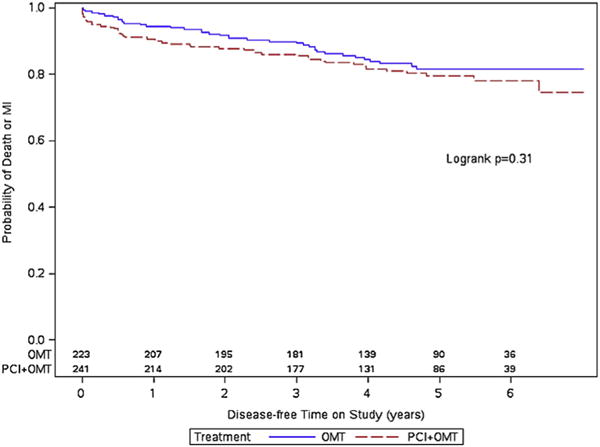
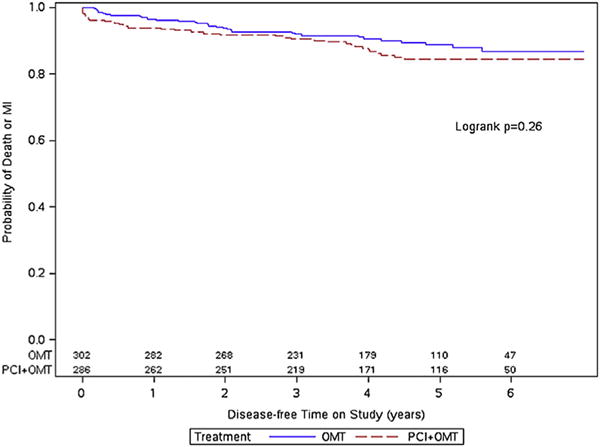
The impact of baseline exercise capacity on clinical outcomes in patients with stable ischemic heart disease randomized to an initial strategy of optimal medical therapy (OMT) with or without percutaneous coronary intervention (PCI) in the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial has not been studied. A post hoc analysis was performed in 1,052 patients of COURAGE (PCI + OMT: n = 527, OMT: n = 525) who underwent exercise treadmill testing at baseline. Patients were categorized into 2 exercise capacity groups based on metabolic equivalents (METs) achieved during baseline exercise treadmill testing (<7 METs: n = 464, ≥7 METs: n = 588) and were followed for a median of 4.6 years. The primary composite end point of death or myocardial infarction was similar in the PCI + OMT group and the OMT group for patients with exercise capacity <7 METs (19.1% vs 16.1%, p = 0.31) and ≥7 METs (13.3% vs 10.3%, p = 0.27). After adjusting for baseline covariates, the hazard ratio (99% confidence interval) for the primary end point for the PCI + OMT group versus the OMT group was 1.42 (0.90 to 2.23, p = 0.05) and for the exercise capacity subgroups of ≥7 METs and <7 METs was 0.75 (0.46 to 1.22, p = 0.13). There was no statistically significant interaction between the original treatment arm allocation (PCI + OMT vs OMT) and baseline exercise capacity. In conclusion, there was no difference in the long-term clinical outcomes in patients with exercise capacity <7 METs compared with ≥7 METs, irrespective of whether they were assigned to initial PCI. Patients with exercise capacity <7 METs did not derive a proportionately greater clinical benefit from PCI + OMT compared with those patients who received OMT alone.
在“利用血运重建和强化药物评估的临床结果(COURAGE)”试验中,对于随机接受初始最佳药物治疗(OMT)策略(无论是否进行经皮冠状动脉介入治疗(PCI))的稳定型缺血性心脏病患者,基线运动能力对临床结果的影响尚未得到研究。对COURAGE试验中1052例在基线时进行运动平板试验的患者进行了事后分析(PCI + OMT组:n = 527,OMT组:n = 525)。根据基线运动平板试验期间达到的代谢当量(METs),将患者分为2个运动能力组(<7 METs:n = 464,≥7 METs:n = 588),并随访了4.6年的中位数时间。对于运动能力<7 METs的患者,PCI + OMT组和OMT组的主要复合终点死亡或心肌梗死相似(19.1%对16.1%,p = 0.31);对于运动能力≥7 METs的患者,也是如此(13.3%对10.3%,p = 0.27)。在对基线协变量进行调整后,PCI + OMT组与OMT组相比,主要终点的风险比(99%置信区间)为1.42(0.90至2.23,p = 0.05),对于运动能力≥7 METs和<7 METs的亚组,风险比为0.75(0.46至1.22,p = 0.13)。原始治疗组分配(PCI + OMT与OMT)与基线运动能力之间没有统计学上的显著相互作用。总之,表示,无论患者是否被分配接受初始PCI,运动能力<7 METs的患者与≥7 METs的患者相比,长期临床结果没有差异。与仅接受OMT的患者相比,运动能力<7 METs的患者并未从PCI + OMT中获得成比例更大的临床益处。