Camiciottoli Gianna, Diciotti Stefano, Bigazzi Francesca, Lombardo Simone, Bartolucci Maurizio, Paoletti Matteo, Mascalchi Mario, Pistolesi Massimo
Section of Respiratory Medicine, Department of Clinical and Experimental Medicine, University of Florence, Florence, Italy.
Department of Electrical, Electronic, and Information Engineering "Guglielmo Marconi," University of Bologna, Cesena, Italy.
Int J Chron Obstruct Pulmon Dis. 2015 Apr 28;10:843-52. doi: 10.2147/COPD.S80558. eCollection 2015.
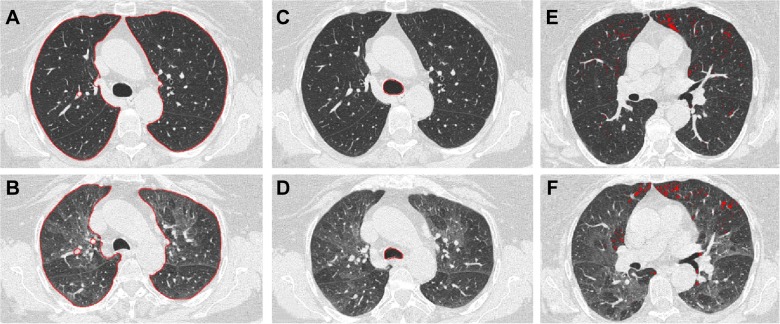
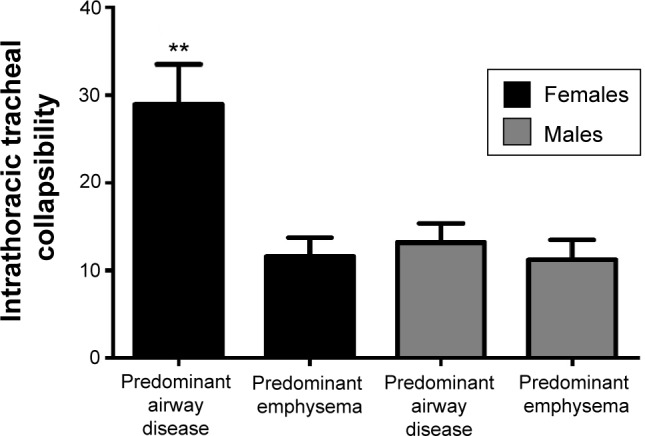
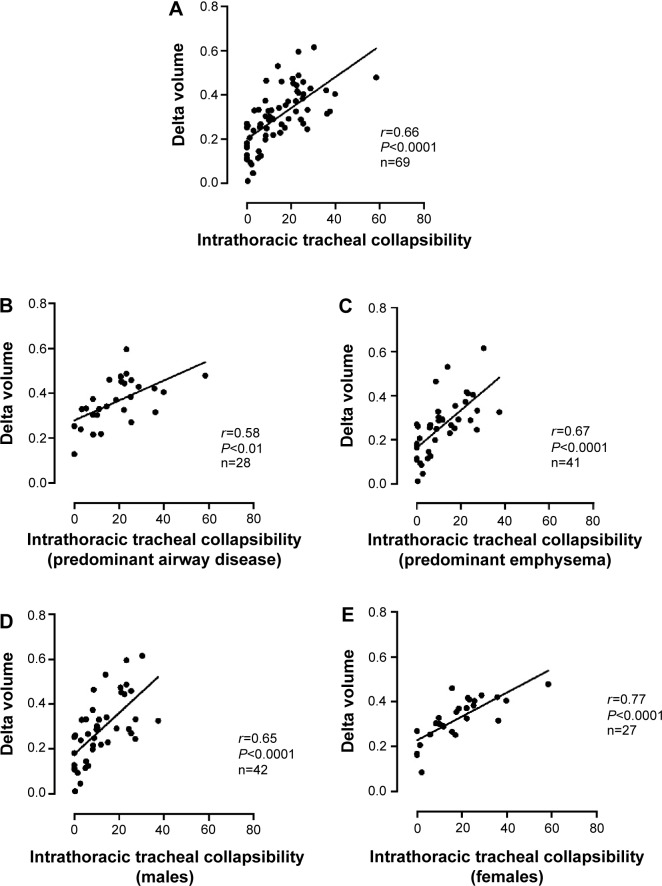
A substantial proportion of patients with chronic obstructive pulmonary disease (COPD) develops various degree of intrathoracic tracheal collapsibility. We studied whether the magnitude of intrathoracic tracheal collapsibility could be different across clinical phenotypes and sex in COPD. Intrathoracic tracheal collapsibility measured at paired inspiratory-expiratory low dose computed tomography (CT) and its correlation with clinical, functional, and CT-densitometric data were investigated in 69 patients with COPD according to their predominant conductive airway or emphysema phenotypes and according to sex. Intrathoracic tracheal collapsibility was higher in patients with predominant conductive airway disease (n=28) and in females (n=27). Women with a predominant conductive airway phenotype (n=10) showed a significantly greater degree of collapsibility than women with predominant emphysema (28.9%±4% versus 11.6%±2%; P<0.001). Intrathoracic tracheal collapsibility was directly correlated with inspiratory-expiratory volume variation at CT and with forced expiratory volume (1 second), and inversely correlated with reduced CT lung density and functional residual capacity. Intrathoracic tracheal collapsibility was not correlated with cough and wheezing; however, intrathoracic tracheal collapsibility and clinical phenotypes of COPD are closely correlated. In patients with a predominant emphysematous phenotype, a reduced collapsibility may reflect the mechanical properties of the stiff hyperinflated emphysematous lung. The high collapsibility in patients with predominant airway disease, mild airway obstruction, and in women with this phenotype may reflect chronic airway inflammation. The lack of relationship with such symptoms as wheezing, cough, and dyspnea could indicate that intrathoracic tracheal collapsibility itself should be considered neither an abnormal feature of COPD nor a relevant clinical finding.
相当一部分慢性阻塞性肺疾病(COPD)患者会出现不同程度的胸内气管塌陷。我们研究了COPD患者胸内气管塌陷程度在临床表型和性别上是否存在差异。根据主要的传导气道或肺气肿表型以及性别,对69例COPD患者进行了吸气 - 呼气低剂量计算机断层扫描(CT)测量的胸内气管塌陷程度及其与临床、功能和CT密度测定数据的相关性研究。主要表现为传导气道疾病的患者(n = 28)和女性患者(n = 27)的胸内气管塌陷程度更高。以传导气道表型为主的女性患者(n = 10)的塌陷程度明显高于以肺气肿为主的女性患者(28.9%±4%对11.6%±2%;P<0.001)。胸内气管塌陷程度与CT上的吸气 - 呼气容积变化以及用力呼气容积(1秒)直接相关,与CT肺密度降低和功能残气量呈负相关。胸内气管塌陷程度与咳嗽和喘息无关;然而,胸内气管塌陷程度与COPD的临床表型密切相关。在以肺气肿表型为主的患者中,塌陷程度降低可能反映了僵硬的过度充气肺气肿肺的力学特性。以气道疾病为主、轻度气道阻塞的患者以及具有这种表型的女性患者中塌陷程度较高,可能反映了慢性气道炎症。与喘息、咳嗽和呼吸困难等症状缺乏相关性可能表明,胸内气管塌陷本身既不应被视为COPD的异常特征,也不应被视为相关的临床发现。