Sayal Karen, Gounaris Ioannis, Basu Bristi, Freeman Sue, Moyle Penny, Hosking Karen, Iddawela Mahesh, Jimenez-Linan Mercedes, Abraham Jean, Brenton James, Hatcher Helen, Earl Helena, Parkinson Christine
*Department of Oncology, Cambridge University NHS Foundation Trust, Cambridge, United Kingdom; †Cancer Research United Kingdom Cambridge Institute, University of Cambirdge, Li Ka Shing Centre, Cambridge, United Kingdom; ‡Department of Radiology, Cambridge University NHS Foundation Trust, Cambridge, United Kingdom; §Department of Oncology, University of Cambridge, Cambridge, United Kingdom; and ∥Department of Histopathology, Cambridge University NHS Foundation Trust, Cambridge, United Kingdom.
Int J Gynecol Cancer. 2015 Jul;25(6):977-84. doi: 10.1097/IGC.0000000000000448.
Primary platinum-resistant epithelial ovarian cancer (EOC) is an area of unmet medical need. There is limited evidence from small studies that platinum-based combinations can overcome "resistance" in a proportion of patients. We investigated the efficacy and toxicity of platinum-based combination chemotherapy in the platinum-resistant and platinum-refractory setting.
Epirubicin, cisplatin, and capecitabine (ECX) combination chemotherapy was used at our institution for the treatment of relapsed EOC. From the institutional database, we identified all patients with primary platinum-refractory or platinum-resistant relapse treated with ECX as second-line therapy between 2001 and 2012. We extracted demographic, clinical, treatment, and toxicity data and outcomes. We used logistic and Cox regression models to identify predictors of response and survival respectively.
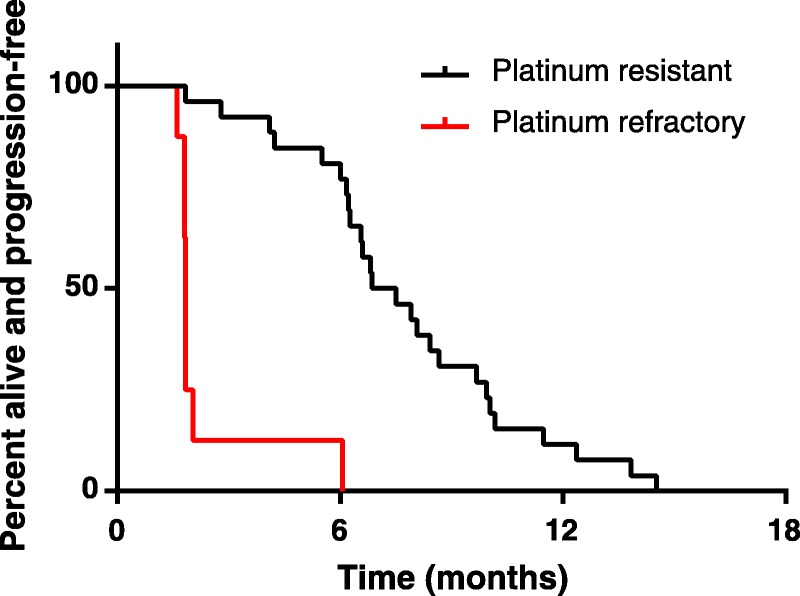
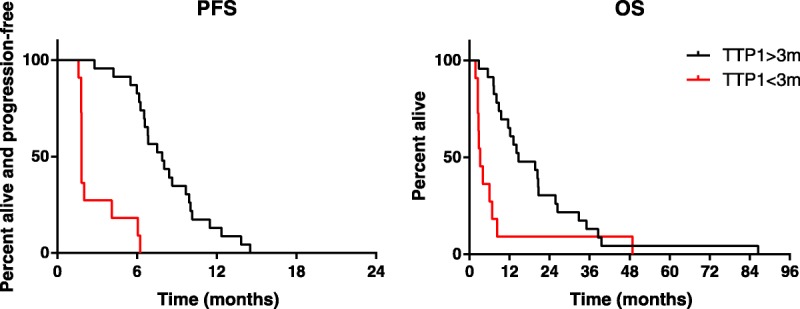
Thirty-four 34 patients (8 refractory, 26 resistant) were treated with ECX. Response Evaluation Criteria In Solid Tumors (RECIST) response rate was 45%, median progression-free survival (PFS) was 6.4 months, and overall survival (OS) was 10.6 months. Platinum-resistant patients had better outcomes than did platinum-refractory patients (response rate, 54% vs 0%, P = 0.047; PFS 7.2 vs 1.8 months, P < 0.0001; OS 14.4 vs 3 months, P < 0.001). In regression models, time to progression after first-line treatment and platinum-refractory status were the strongest predictors of response and PFS or OS, respectively. Patients with time to progression after first-line treatment longer than 3 months showed PFS and OS of 7.9 and 14.7 months, respectively. Toxicity was manageable, with only 13% of cycles administered at reduced doses.
Epirubicin, cisplatin, and capecitabine seems to be active in platinum-resistant relapsed EOC with manageable toxicity. Further prospective investigation of platinum-anthracycline combinations is warranted in patients who relapse 3 to 6 months after first-line platinum-taxane treatment.
原发性铂耐药上皮性卵巢癌(EOC)是一个尚未满足医学需求的领域。小型研究的证据有限,表明铂类联合方案能使一部分患者克服“耐药性”。我们调查了铂类联合化疗在铂耐药和铂难治情况下的疗效及毒性。
我院使用表柔比星、顺铂和卡培他滨(ECX)联合化疗治疗复发性EOC。从机构数据库中,我们确定了2001年至2012年间所有接受ECX作为二线治疗的原发性铂难治或铂耐药复发患者。我们提取了人口统计学、临床、治疗、毒性数据及结果。我们分别使用逻辑回归和Cox回归模型来确定反应和生存的预测因素。
34例患者(8例难治,26例耐药)接受了ECX治疗。实体瘤疗效评价标准(RECIST)反应率为45%,中位无进展生存期(PFS)为6.4个月,总生存期(OS)为10.6个月。铂耐药患者的结局优于铂难治患者(反应率,54%对0%,P = 0.047;PFS 7.2对1.8个月,P < 0.0001;OS 14.4对3个月,P < 0.001)。在回归模型中,一线治疗后至进展时间和铂难治状态分别是反应及PFS或OS的最强预测因素。一线治疗后至进展时间超过3个月的患者,PFS和OS分别为7.9个月和14.7个月。毒性可控,仅13%的周期采用了减量给药。
表柔比星、顺铂和卡培他滨似乎对铂耐药复发性EOC有效,且毒性可控。对于一线铂类紫杉烷治疗后3至6个月复发的患者,有必要进一步对铂类-蒽环类联合方案进行前瞻性研究。