Wagenaar Inge, van Muiden Lisanne, Alam Khorshed, Bowers Robert, Hossain Md Anwar, Kispotta Kolpona, Richardus Jan Hendrik
Department of Public Health, Erasmus Medical Center, Rotterdam, The Netherlands.
Wageningen University and Research Centre, Wageningen, The Netherlands.
PLoS Negl Trop Dis. 2015 May 12;9(5):e0003766. doi: 10.1371/journal.pntd.0003766. eCollection 2015 May.
Food shortage was associated with leprosy in two recent studies investigating the relation between socioeconomic factors and leprosy. Inadequate intake of nutrients due to food shortage may affect the immune system and influence the progression of infection to clinical leprosy. We aimed to identify possible differences in dietary intake between recently diagnosed leprosy patients and control subjects.
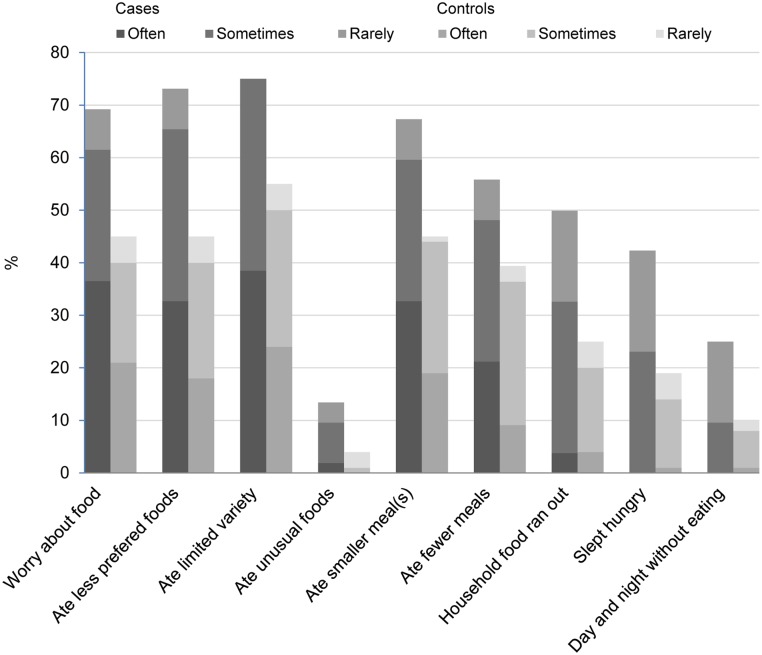
In a leprosy endemic area of Bangladesh, newly diagnosed leprosy patients and control subjects were interviewed about their socioeconomic situation, health and diet. Dietary intakes were recorded with a 24-hour recall, from which a Dietary Diversity Score (DDS) was calculated. Body Mass Index (BMI) was calculated and Household Food Insecurity Access Scale (HFIAS) was filled out for every participant. Using logistic regression, a univariate, block wise multivariate, and an integrated analysis were carried out.
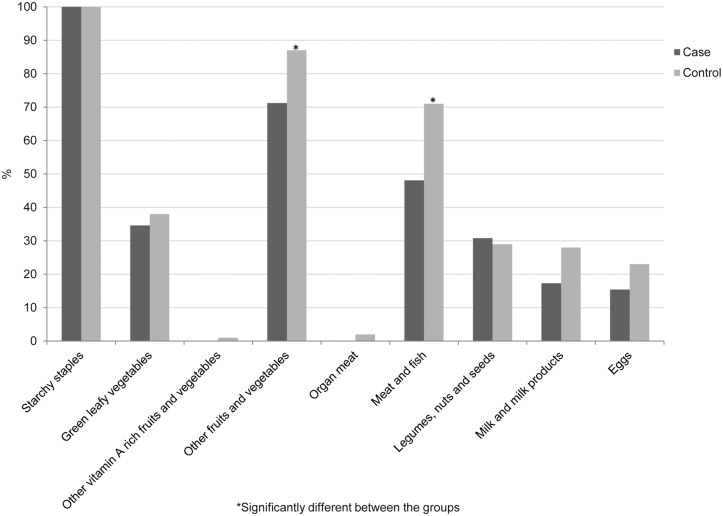
52 leprosy cases and 100 control subjects were included. Food shortage was more common, dietary diversity was lower and household food insecurity was higher in the patient group. Patients consumed significantly less items from the DDS food groups 'Meat and fish' and 'Other fruits and vegetables.' Lower food expenditure per capita, lower BMI, lower DDS and absence of household food stocks are the main factors associated with an increased risk of having leprosy.
Low income families have only little money to spend on food and consequently have a low intake of highly nutritious non-rice foods such as meat, fish, milk, eggs, fruits and vegetables. Development of clinical leprosy could be explained by deficiencies of the nutrients that these foods normally provide.
在最近两项调查社会经济因素与麻风病关系的研究中,食物短缺与麻风病有关。由于食物短缺导致的营养摄入不足可能会影响免疫系统,并影响感染向临床麻风病的进展。我们旨在确定新诊断的麻风病患者与对照受试者在饮食摄入方面可能存在的差异。
在孟加拉国的一个麻风病流行地区,对新诊断的麻风病患者和对照受试者进行了关于他们的社会经济状况、健康和饮食的访谈。通过24小时回顾法记录饮食摄入量,并据此计算饮食多样性得分(DDS)。计算每个参与者的体重指数(BMI),并填写家庭粮食不安全获取量表(HFIAS)。使用逻辑回归进行单变量、逐块多变量和综合分析。
纳入了52例麻风病病例和100名对照受试者。患者组食物短缺更为常见,饮食多样性较低,家庭粮食不安全程度较高。患者从DDS食物组“肉类和鱼类”以及“其他水果和蔬菜”中摄入的食物明显较少。人均食品支出较低、BMI较低、DDS较低以及家庭没有粮食储备是与患麻风病风险增加相关的主要因素。
低收入家庭在食物上的支出很少,因此对肉类、鱼类、牛奶、鸡蛋、水果和蔬菜等高营养非大米类食物的摄入量较低。临床麻风病的发生可能是由于这些食物通常提供的营养素缺乏所致。