Jalaeikhoo Hasan, Khajeh-Mehrizi Ahmad
AJA cancer research center (ACRC), AJA University of Medical Sciences, Tehran, Iran.
PLoS One. 2015 May 13;10(5):e0126925. doi: 10.1371/journal.pone.0126925. eCollection 2015.
Aplastic anemia (AA) is a rare disease in which hematopoietic stem cells are severely diminished resulting in hypocellular bone marrow and pancytopenia. Etiology of AA includes auto immunity, toxins, infection, ionizing radiation, drugs and rare genetic disorders, but in the majority of cases no cause can be identified. In the present study we assessed response rate, survival, relapse and clonal evolution in patients with AA treated with immunosuppressive therapy.
Patients with AA who received immunosuppressive therapy between May 1998 and September 2013 were included in this study. Patients with non-severe AA (NSAA) were treated with cyclosporine (CsA) and danazol while patients with severe AA (SAA) as well as patients with NSAA who progressed to SAA after beginning of the treatment, were candidates for receiving antithymocyte globulin in addition to CsA and danazol.
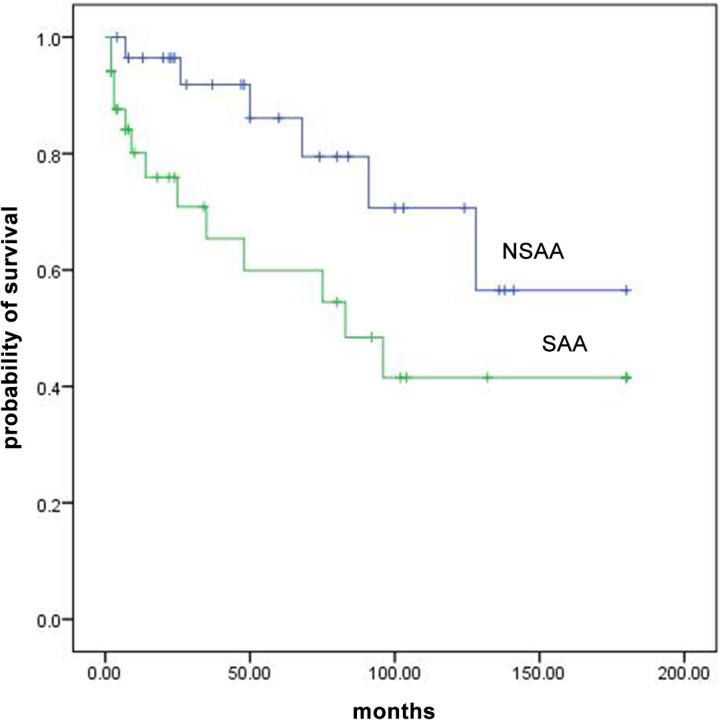
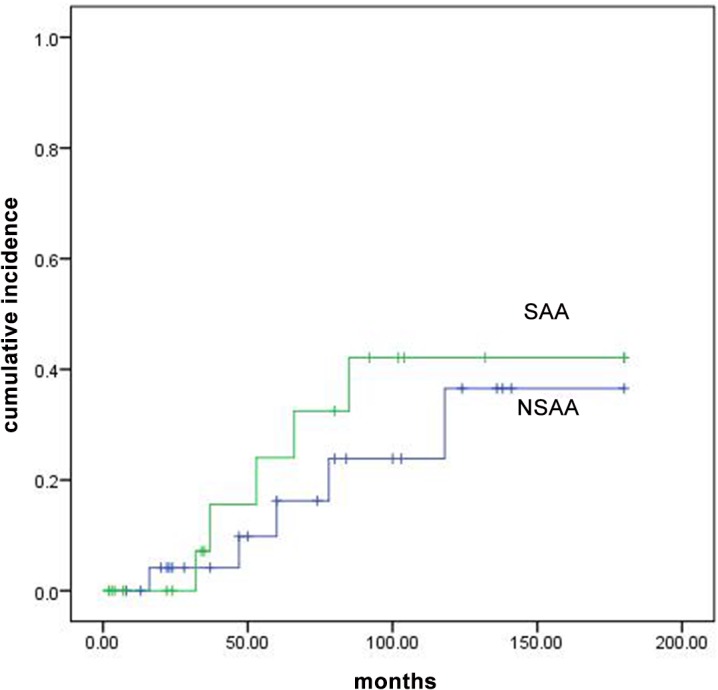
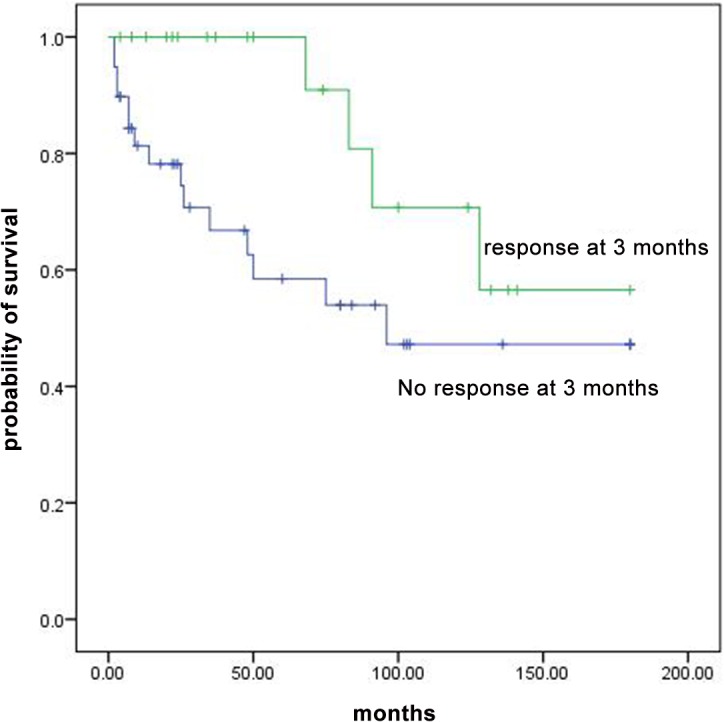
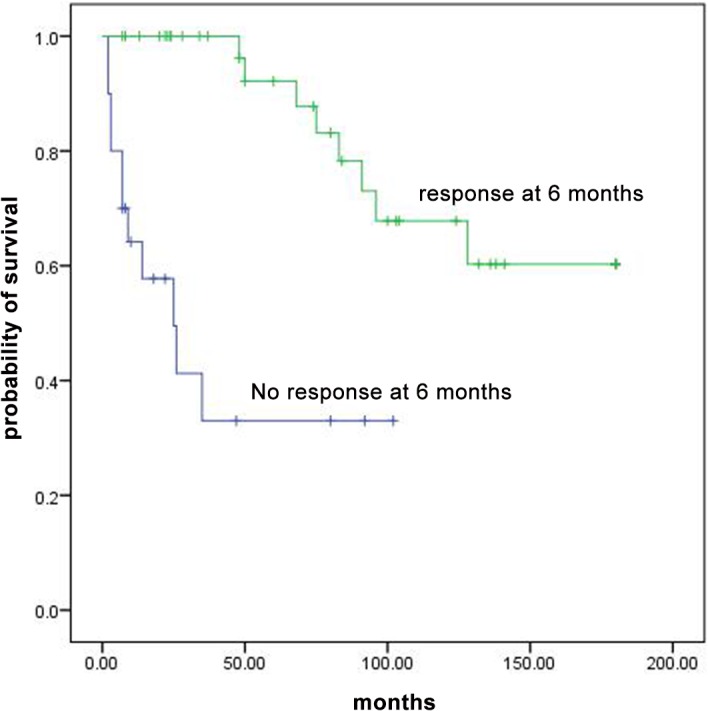
Among the 63 studied patients, 29 (46%) had NSAA and 34 (54%) had SAA. Three months after treatment, overall response was 58.6% in NSAA and 12.9% in patients with SAA. Survival of all patients at 5, 10 and 15 years were 73%, 55% and 49%, respectively. Survival rates were significantly higher in patients with NSAA compared to patients with SAA as well as in patients who responded at 6 months compared to non-responders. The relapse risk was 39.7% at 10 years. Relapse occurred in patients who discontinued the therapy more than those who continued taking CsA (p value<0.01). The risk of clonal evolution was 9.9% at 10 years and 22.8% at 15 years after treatment.
This long-term retrospective study indicated that immunosuppressive therapy should be recommended to patients with AA. Also, our experience indicated that immunosuppressive therapy should not be discontinued after response to therapy in patients with both NSAA and SAA due to high risk of relapse. Low dose of CsA should be continued indefinitely.
再生障碍性贫血(AA)是一种罕见疾病,造血干细胞严重减少,导致骨髓细胞减少和全血细胞减少。AA的病因包括自身免疫、毒素、感染、电离辐射、药物和罕见的遗传疾病,但在大多数情况下无法确定病因。在本研究中,我们评估了接受免疫抑制治疗的AA患者的缓解率、生存率、复发率和克隆演变情况。
本研究纳入了1998年5月至2013年9月期间接受免疫抑制治疗的AA患者。非重型AA(NSAA)患者接受环孢素(CsA)和达那唑治疗,而重型AA(SAA)患者以及治疗开始后进展为SAA的NSAA患者,除CsA和达那唑外,还接受抗胸腺细胞球蛋白治疗。
在63例研究患者中,29例(46%)为NSAA,34例(54%)为SAA。治疗3个月后,NSAA患者的总体缓解率为58.6%,SAA患者为12.9%。所有患者5年、10年和15年的生存率分别为73%、55%和49%。与SAA患者相比,NSAA患者的生存率显著更高,与未缓解患者相比,6个月时缓解患者的生存率也显著更高。10年时的复发风险为39.7%。与继续服用CsA的患者相比,停药患者的复发率更高(p值<0.01)。治疗后10年的克隆演变风险为9.9%,15年为22.8%。
这项长期回顾性研究表明,AA患者应推荐免疫抑制治疗。此外,我们的经验表明,由于复发风险高,NSAA和SAA患者在治疗缓解后不应停止免疫抑制治疗。应无限期持续使用低剂量的CsA。