Boddu Prajwal, Garcia-Manero Guillermo, Ravandi Farhad, Borthakur Gautam, Jabbour Elias, DiNardo Courtney, Jain Nitin, Daver Naval, Pemmaraju Naveen, Anderlini Paolo, Parmar Simrit, Kc Devendra, Akosile Mary, Pierce Sherry A, Champlin Richard, Cortes Jorge, Kantarjian Hagop, Kadia Tapan
Departments of Leukemia, The University of Texas, M. D. Anderson Cancer Center, Houston, Texas.
Stem Cell Transplant, The University of Texas, M. D. Anderson Cancer Center, Houston, Texas.
Am J Hematol. 2017 Dec;92(12):1295-1302. doi: 10.1002/ajh.24897. Epub 2017 Sep 25.
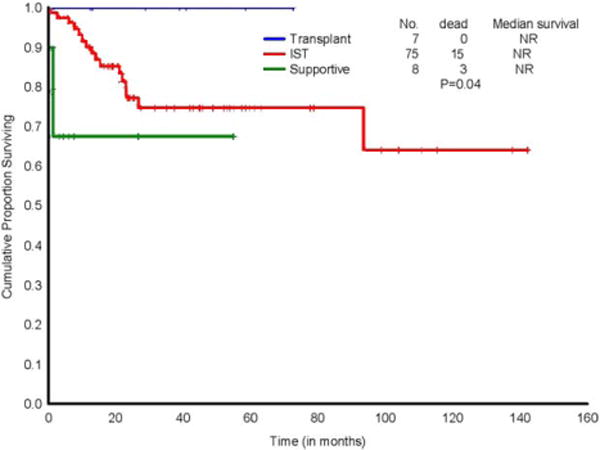
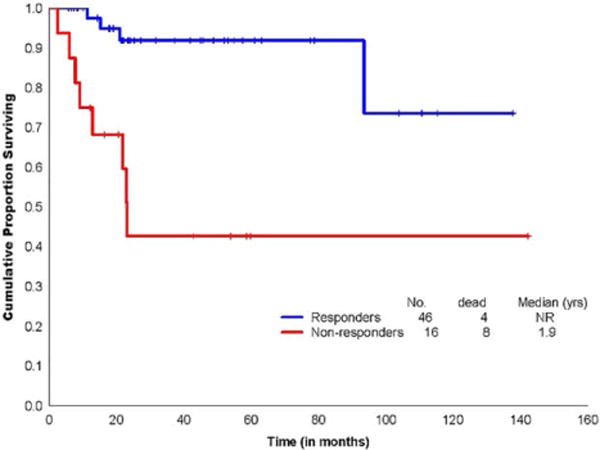
Newer treatment modalities are being investigated to improve upon historical outcomes with standard immunosuppressive therapy (IST) in aplastic anemia (AA). We analyzed outcomes of adult patients with AA treated with various combinatorial anti-thymoglobulin-based IST regimens in frontline and relapsed/refractory (R/R) settings. Pretreatment and on-treatment clinical characteristics were analyzed for relationships to response and outcome. Among 126 patients reviewed, 95 were treatment-naïve (TN) and 63, R/R (including 32 from the TN cohort); median ages were 49 and 50 years, respectively. Overall survival (OS) was superior in IST responders (P < .001). Partial response to IST was associated with shorter relapse-free survival (RFS), as compared with complete response (P = .03). By multivariate analysis, baseline platelet and lymphocyte count predicted for IST response at 3 and 6 months, respectively. While additional growth factor interventions led to faster count recovery, there were no statistically significant differences in RFS or OS across the various frontline IST regimens (i.e., with/without G-CSF or eltrombopag). While marrow cellularity did not correlate with peripheral-blood counts at 3 months, cytomorphological assessment revealed dyspoietic changes in all nonresponders with hypercellular-marrow indices. Covert dysplasia, identified through early bone marrow assessment, has implications on future therapy choices after IST failure. Salvage IST response depended upon prior response to ATG: prior responders (46%) vs. primary refractory (0%) (P < .01). In the R/R setting, there was no survival difference between IST and allogeneic stem cell transplant groups, with a trend toward superior OS in the former. Transplant benefits in the R/R setting may be underrealized due to transplant-related mortality.
目前正在研究更新的治疗方式,以改善再生障碍性贫血(AA)患者接受标准免疫抑制治疗(IST)时的历史疗效。我们分析了成年AA患者在一线治疗以及复发/难治性(R/R)情况下接受各种基于抗胸腺细胞球蛋白的联合IST方案治疗的疗效。分析了预处理和治疗期间的临床特征与反应及疗效之间的关系。在126例接受评估的患者中,95例为初治患者(TN),63例为复发/难治性患者(包括32例来自TN队列);中位年龄分别为49岁和50岁。IST反应者的总生存期(OS)更长(P < 0.001)。与完全缓解相比,IST部分缓解与无复发生存期(RFS)较短相关(P = 0.03)。多因素分析显示,基线血小板计数和淋巴细胞计数分别可预测3个月和6个月时的IST反应。虽然额外的生长因子干预可使血细胞计数恢复更快,但不同一线IST方案(即使用/不使用粒细胞集落刺激因子或艾曲泊帕)的RFS或OS无统计学显著差异。虽然3个月时骨髓细胞计数与外周血计数不相关,但细胞形态学评估显示,所有骨髓细胞计数高且无反应的患者均有发育异常改变。通过早期骨髓评估发现的隐匿性发育异常对IST失败后的未来治疗选择有影响。挽救性IST反应取决于先前对抗胸腺细胞球蛋白的反应:先前有反应者(46%)与原发难治者(0%)(P < 0.01)。在R/R情况下,IST组和异基因干细胞移植组的生存率无差异,前者有OS更高的趋势。由于移植相关死亡率,R/R情况下的移植益处可能未得到充分实现。