Mc Causland Finnian R, Waikar Sushrut S
Renal Division, Department of Medicine, Brigham and Women's Hospital, Boston, MA; Harvard Medical School, Boston, MA.
Renal Division, Department of Medicine, Brigham and Women's Hospital, Boston, MA; Harvard Medical School, Boston, MA.
Am J Kidney Dis. 2015 Sep;66(3):499-506. doi: 10.1053/j.ajkd.2015.03.028. Epub 2015 May 12.
The rapid reduction in plasma osmolality during hemodialysis (HD) may induce temporary gradients that promote the movement of water from the extracellular to the intracellular compartment, predisposing to the development of intradialytic hypotension (IDH).
Observational cohort study.
SETTING & PARTICIPANTS: 3,142 prevalent patients receiving thrice-weekly HD from a single dialysis provider organization.
Predialysis calculated plasma osmolarity (calculated after the 2-day interval as 2 × serum sodium + serum urea nitrogen/2.8 + serum glucose/18).
Magnitude of systolic blood pressure (SBP) decline (predialysis SBP - nadir intradialytic SBP) and risk of IDH (SBP decline > 35 or nadir SBP < 90 mm Hg).
Unadjusted and multivariable-adjusted generalized linear models were fit to estimate the association of calculated osmolarity with intradialytic SBP decline and the odds of developing IDH.
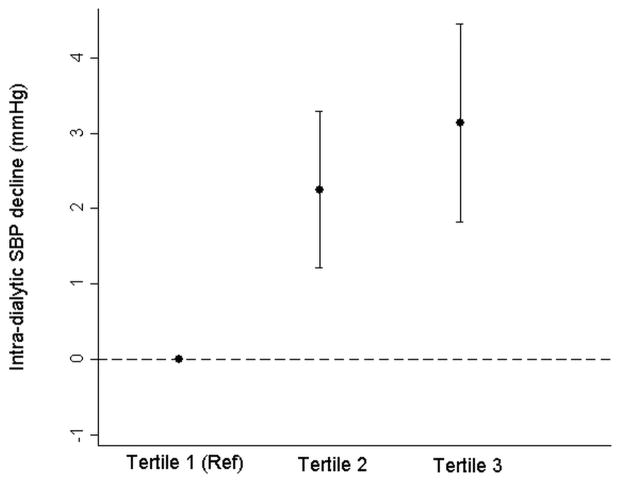
Mean age of participants was 62.6±15.2 (SD) years, 57.1% were men, and 61.0% had diabetes. Mean predialysis calculated osmolarity during follow-up was 306.4 ± 9.5 mOsm/L. After case-mix adjustment, each 10-mOsm/L increase in predialysis calculated osmolarity was associated with 1.48 (95% CI, 0.86-2.09) mm Hg (P < 0.001) greater decline in intradialytic SBP and 10% greater odds of IDH (OR, 1.10; 95% CI, 1.05-1.15). In adjusted models, lower predialysis sodium and higher serum urea nitrogen and serum glucose levels were associated with greater decline in intradialytic SBP.
Measured serum osmolality, timing of changes in intradialytic osmolality, dialysate osmolality, and dialysate temperature were not available.
Higher predialysis calculated osmolarity is associated with greater decline in intradialytic SBP and greater risk of IDH in maintenance HD patients. Strategies to minimize rapid shifts in osmolality should be tested prospectively to minimize excess SBP decline in susceptible patients.
血液透析(HD)期间血浆渗透压的快速降低可能会诱导暂时性梯度,促使水从细胞外间隙向细胞内间隙移动,从而易引发透析中低血压(IDH)。
观察性队列研究。
来自单一透析服务机构的3142例接受每周三次HD的长期透析患者。
透析前计算的血浆渗透压(间隔2天后计算,公式为2×血清钠+血清尿素氮/2.8+血清葡萄糖/18)。
收缩压(SBP)下降幅度(透析前SBP - 透析中SBP最低点)和IDH风险(SBP下降>35或SBP最低点<90 mmHg)。
采用未调整和多变量调整的广义线性模型来估计计算渗透压与透析中SBP下降以及发生IDH几率之间的关联。
参与者的平均年龄为62.6±15.2(标准差)岁,57.1%为男性,61.0%患有糖尿病。随访期间透析前计算的平均渗透压为306.4±9.5 mOsm/L。在进行病例组合调整后,透析前计算渗透压每升高10 mOsm/L,与透析中SBP下降幅度增加1.48(95%可信区间,0.86 - 2.09)mmHg(P<0.001)以及IDH几率增加10%(比值比,1.10;95%可信区间,1.05 - 1.15)相关。在调整模型中,透析前较低的钠水平以及较高的血清尿素氮和血清葡萄糖水平与透析中SBP下降幅度更大相关。
未获取测量的血清渗透压、透析中渗透压变化的时间、透析液渗透压和透析液温度。
在维持性HD患者中,较高的透析前计算渗透压与透析中SBP下降幅度更大以及IDH风险更高相关。应前瞻性地测试使渗透压快速变化最小化的策略,以尽量减少易感患者的SBP过度下降。