Zhang Eric, Wartelle-Bladou Claire, Lepanto Luigi, Lachaine Jean, Cloutier Guy, Tang An
Department of Radiology, Radio-Oncology and Nuclear Medicine, University of Montreal, Saint-Luc Hospital, Montreal, Quebec, Canada.
Laboratory of Biorheology and Medical Ultrasonics, University of Montreal Hospital Research Center (CRCHUM), Montreal, Quebec, Canada.
Eur Radiol. 2015 Nov;25(11):3282-94. doi: 10.1007/s00330-015-3731-2. Epub 2015 May 21.
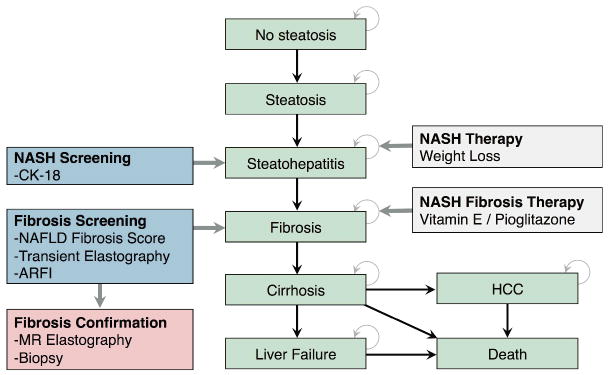
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disease in Western countries. No studies have examined the cost-effectiveness of screening its advanced form, nonalcoholic steatohepatitis (NASH).
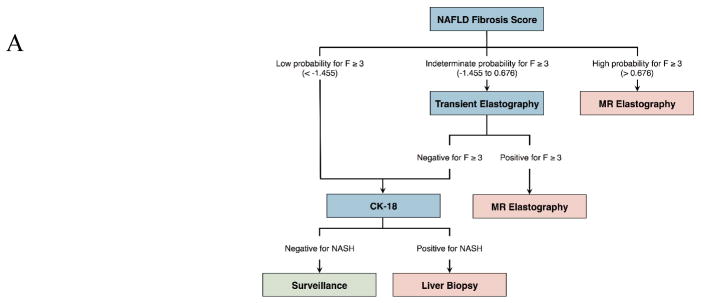
We performed a cost-utility analysis of annual noninvasive screening strategies using third-party payer perspective in a general population in comparison to screening a high-risk obese or diabetic population. Screening algorithms involved well-studied techniques, including NAFLD fibrosis score, transient elastography (TE), and acoustic radiation force impulse (ARFI) imaging for detecting advanced fibrosis (≥ F3); and plasma cytokeratin (CK)-18 for NASH detection. Liver biopsy and magnetic resonance elastography (MRE) were compared as confirmation methods. Canadian dollar (CAD or C$) costs were adjusted for inflation and discounted at 5%. Incremental cost-effectiveness ratio (ICER) of ≤C$ 50,000 was considered cost-effective.
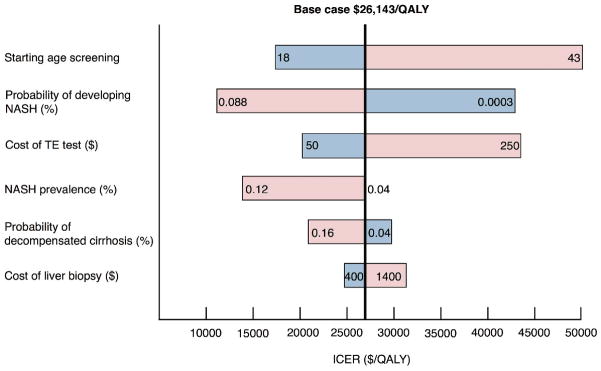
Compared with no screening, screening with NAFLD fibrosis score/TE/CK-18 algorithm with MRE as confirmation for advanced fibrosis had an ICER of C$ 26,143 per quality-adjusted life year (QALY) gained. Screening in high-risk obese or diabetic populations was more cost-effective, with an ICER of C$ 9,051 and C$ 7,991 per quality-adjusted life-year (QALY) gained, respectively. Liver biopsy confirmation was not found to be cost-effective.
Our model suggests that annual NASH screening in high-risk obese or diabetic populations can be cost-effective.
• This cost-utility analysis suggests that screening for nonalcoholic steatohepatitis may be cost-effective. • In particular, screening of high-risk obese or diabetic populations is more cost-effective. • Magnetic resonance elastography was more cost-effective to confirm disease compared to biopsy. • More studies are needed to determine quality of life in nonalcoholic steatohepatitis. • More management strategies for nonalcoholic steatohepatitis are also needed.
非酒精性脂肪性肝病(NAFLD)是西方国家最常见的肝脏疾病。尚无研究探讨筛查其晚期形式非酒精性脂肪性肝炎(NASH)的成本效益。
我们采用第三方支付方视角,对普通人群的年度非侵入性筛查策略与筛查高危肥胖或糖尿病患者人群进行了成本效用分析。筛查算法涉及经过充分研究的技术,包括用于检测晚期纤维化(≥F3)的NAFLD纤维化评分、瞬时弹性成像(TE)和声辐射力脉冲(ARFI)成像;以及用于检测NASH的血浆细胞角蛋白(CK)-18。将肝活检和磁共振弹性成像(MRE)作为确认方法进行比较。以加元(CAD或C$)计算的成本进行了通货膨胀调整,并按5%进行贴现。增量成本效益比(ICER)≤50,000加元被认为具有成本效益。
与不进行筛查相比,采用NAFLD纤维化评分/TE/CK-18算法并以MRE确认晚期纤维化的筛查每获得一个质量调整生命年(QALY)的ICER为26,143加元。在高危肥胖或糖尿病患者人群中进行筛查更具成本效益,每获得一个质量调整生命年(QALY)的ICER分别为9,051加元和7,991加元。未发现肝活检确认具有成本效益。
我们的模型表明,对高危肥胖或糖尿病患者人群进行年度NASH筛查可能具有成本效益。
• 这项成本效用分析表明,筛查非酒精性脂肪性肝炎可能具有成本效益。• 特别是,筛查高危肥胖或糖尿病患者人群更具成本效益。• 与活检相比,磁共振弹性成像在确认疾病方面更具成本效益。• 需要更多研究来确定非酒精性脂肪性肝炎患者的生活质量。• 还需要更多针对非酒精性脂肪性肝炎的管理策略。