Saberian Arash, Dehghan Azizallah, Homayounfar Reza, Kaffashan Saeid, Zarei Fariba, Niknejad Sepideh, Farjam Mojtaba
Medical Imaging Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
Department of Epidemiology, Noncommunicable Diseases Research Center, Fasa University of Medical Sciences, Fasa, Iran.
BMC Gastroenterol. 2024 Dec 2;24(1):443. doi: 10.1186/s12876-024-03535-x.
Non-alcoholic fatty liver disease (NAFLD) is a common chronic liver disease in human history and it is expected to surpass other causes of liver disease mortality by 2030. Therefore, finding an alternative way to diagnose steatosis in the early stage when imaging modalities are not available is crucial. This study decided to validate the optimal cut-off points and the sensitivity and specificity of the Fatty Liver Index (FLI) based on the Iranian population compared to ultrasonography.
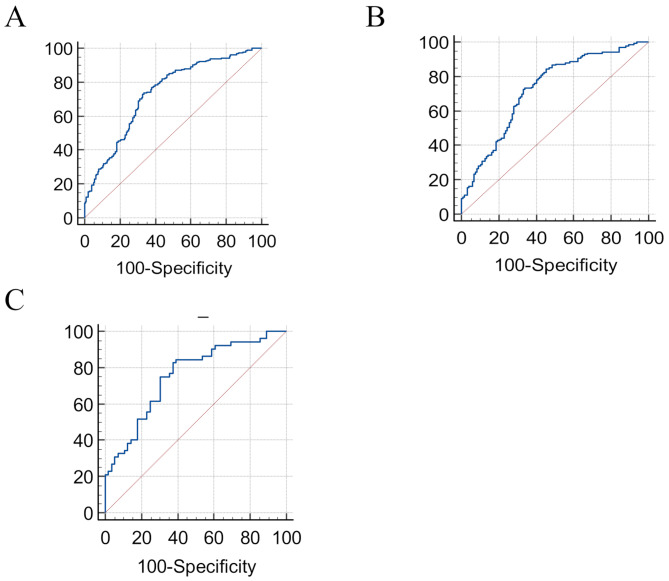
The data of 367 individuals, 108 males and 259 females over 35, were analyzed. Hepatic steatosis was identified by ultrasound. FLI was determined from waist circumference, gamma-glutamyl transferase, triglyceride, and body mass index data. The receiver operating characteristic curve (ROC) was used to determine the best FLI index cut point for diagnosing nonalcoholic fatty liver. The sensitivity and specificity indices were calculated for the determined cut point.
The AUC of the FLI index in diagnosing NAFLD in the total population was 0.733 (95% CI: 0.68-0.77, specificity = 0.6705, sensitivity = 0.7320) with the optimal COP of 40.6. There was a statistically significant association between non-alcoholic liver disease and FLI-based ultrasound (p < 0.0001). Furthermore, the sex-specific optimal COPs of FLI was 33.4, specificity = 0.6071, sensitivity = 0.8462 in men vs. 27.8, sensitivity = 0.8233, specificity = 0.7655 in women.
FLI is a reliable tool for identifying individuals with NAFLD. It has the potential to aid in detecting and managing this condition in large-scale populations while other methods are not available. We also determine an optimal COP of 40.6 with sensitivity and specificity of 73.20% and 67.05% in the general population, respectively.
非酒精性脂肪性肝病(NAFLD)是人类历史上一种常见的慢性肝病,预计到2030年它将超过其他导致肝病死亡的原因。因此,在无法进行影像学检查时找到一种在早期诊断脂肪变性的替代方法至关重要。本研究决定基于伊朗人群验证脂肪肝指数(FLI)相对于超声检查的最佳截断点以及敏感性和特异性。
分析了367名年龄超过35岁的个体的数据,其中男性108名,女性259名。通过超声确定肝脂肪变性。根据腰围、γ-谷氨酰转移酶、甘油三酯和体重指数数据确定FLI。采用受试者工作特征曲线(ROC)来确定诊断非酒精性脂肪肝的最佳FLI指数截断点。计算所确定截断点的敏感性和特异性指数。
FLI指数在总体人群中诊断NAFLD的AUC为0.733(95%CI:0.68 - 0.77,特异性 = 0.6705,敏感性 = 0.7320),最佳截断点为40.6。非酒精性肝病与基于FLI的超声检查之间存在统计学显著关联(p < 0.0001)。此外,FLI的性别特异性最佳截断点在男性中为33.4,特异性 = 0.6071,敏感性 = 0.8462;在女性中为27.8,敏感性 = 0.8233,特异性 = 0.7655。
FLI是识别NAFLD个体的可靠工具。在没有其他方法可用时,它有潜力帮助在大规模人群中检测和管理这种疾病。我们还确定了总体人群中最佳截断点为40.6,敏感性和特异性分别为73.20%和67.05%。