Moeini Mahdi, Khaleghi Ali, Mohammadi Mohammad Reza
Psychiatry and Psychology Research Center, Roozbeh hospital, Tehran University of Medical Sciences, Tehran, Iran.
Department of Biomedical Engineering, Science and Research Branch, Islamic Azad University, Tehran, Iran.
Iran J Psychiatry. 2015;10(1):8-12.
The aim of this study was to compare the QEEG of adolescents affected by bipolar II disorder with age and gender matched healthy controls, and to extract the characteristics of the alpha frequency band to better understand this disorder.
Twenty one adolescents affected by acute episodes of bipolar II disorder (BMD II), both hypomanic and depressive episodes, were selected via convenience sampling based on DSM IV criteria and child and adolescent psychiatrist diagnosis. Eleven patients were going through a hypomanic episode and 10 patients were going through a depression episode. Of the participants, 18 who were matched with the patient group participated in this study as a normal group. Any major comorbidities and intellectual disabilities were excluded through applying K-SADS-PL and Raven's IQ test for all the patients and the healthy participants. Electroencephalogram signals were obtained according to 10-20 international system by 21 electrodes from participants in open and closed eyes in a resting state. We selected 40 seconds length segments from each recorded EEG signals that had minimal noise and artifacts. Power spectrum density (PSD) was estimated for each segment and extracted alpha band frequency. We used only referential (unipolar) montage for comparison. Eventually, data were analyzed by independent Mann-Whitney test and independent t test.
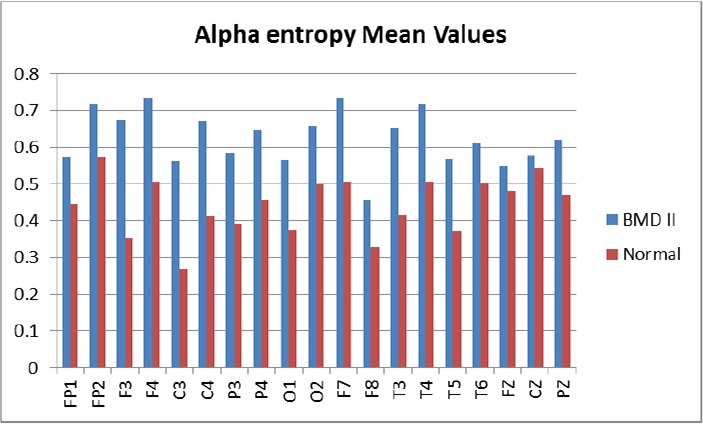
We observed significant differences in the alpha frequency band in some brain regions. Alpha power increased in the fronto-central region and right parietal lobe in the patients (P < 0.05). In the patients with BMD II, entropy of alpha oscillations was larger than the normal participants in the central region and in the F3, F4 and P4 channels. Also, there were differences in the variance of alpha oscillations in these regions between the two groups (P < 0.05). In the occipital lobe, alpha wave had different skewness between the two groups (P < 0.05).
Thalamus as a generator and modulator of at least a part of alpha oscillations may be involved in this disorder and hence this explains the major symptoms like distractibility and inattention in both hypomanic and depressive episodes of bipolar II disorder.
本研究旨在比较双相II型障碍青少年与年龄及性别匹配的健康对照者的定量脑电图(QEEG),并提取阿尔法频段特征,以更好地理解该障碍。
通过便利抽样,依据《精神疾病诊断与统计手册》第四版(DSM-IV)标准及儿童与青少年精神科医生诊断,选取21名受双相II型障碍(BMD II)急性发作影响的青少年,包括轻躁狂发作和抑郁发作。其中11名患者处于轻躁狂发作期,10名患者处于抑郁发作期。18名与患者组匹配的参与者作为正常组参与本研究。通过对所有患者及健康参与者应用儿童版情感障碍和精神分裂症问卷(K-SADS-PL)及瑞文智商测试,排除任何重大共病和智力残疾。根据10-20国际系统,通过21个电极在静息状态下从参与者睁眼和闭眼时获取脑电图信号。我们从每个记录的脑电图信号中选取长度为40秒、噪声和伪迹最小的片段。估计每个片段的功率谱密度(PSD)并提取阿尔法频段频率。我们仅使用参考(单极)导联进行比较。最终,数据通过独立样本曼-惠特尼检验和独立样本t检验进行分析。
我们在一些脑区观察到阿尔法频段存在显著差异。患者额中央区和右侧顶叶的阿尔法功率增加(P < 0.05)。在双相II型障碍患者中,中央区以及F3、F4和P4通道的阿尔法振荡熵大于正常参与者。此外,两组在这些区域的阿尔法振荡方差也存在差异(P < 0.05)。在枕叶,两组之间阿尔法波的偏度不同(P < 0.05)。
丘脑作为至少一部分阿尔法振荡的产生器和调节器,可能参与了该障碍,因此这解释了双相II型障碍轻躁狂和抑郁发作期的主要症状,如注意力分散和注意力不集中。