Beaudoin Amanda, Edison Laura, Introcaso Camille E, Goh Lucy, Marrone James, Mejia Amelita, Van Beneden Chris
MMWR Morb Mortal Wkly Rep. 2015 May 29;64(20):555-8.
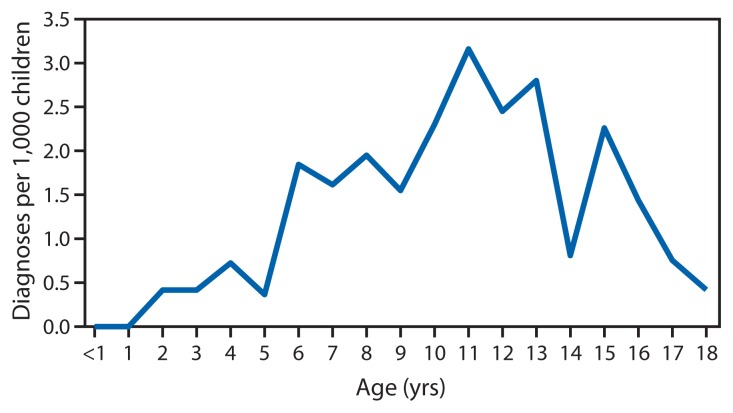
Acute rheumatic fever is a nonsuppurative, immune-mediated consequence of group A streptococcal pharyngitis (strep throat). Recurrent or severe acute rheumatic fever can cause permanent cardiac valve damage and rheumatic heart disease, which increases the risk for cardiac conditions (e.g., infective endocarditis, stroke, and congestive heart failure). Antibiotics can prevent acute rheumatic fever if administered no more than 9 days after symptom onset. Long-term benzathine penicillin G (BPG) injections are effective in preventing recurrent acute rheumatic fever attacks and are recommended to be administered every 3-4 weeks for 10 years or until age 21 years to children who receive a diagnosis of acute rheumatic fever. During August 2013, in response to anecdotal reports of increasing rates of acute rheumatic fever and rheumatic heart disease, CDC collaborated with the American Samoa Department of Health and the Lyndon B. Johnson Tropical Medical Center (the only hospital in American Samoa) to quantify the number of cases of pediatric acute rheumatic fever and rheumatic heart disease in American Samoa and to assess the potential roles of missed pharyngitis diagnosis, lack of timely prophylaxis prescription, and compliance with prescribed BPG prophylaxis. Using data from medical records, acute rheumatic fever incidence was calculated as 1.1 and 1.5 cases per 1,000 children aged ≤18 years in 2011 and 2012, respectively; 49% of those with acute rheumatic fever subsequently received a diagnosis of rheumatic heart disease. Noncompliance with recommended prophylaxis with BPG after physician-diagnosed acute rheumatic fever was noted for 22 (34%) of 65 patients. Rheumatic heart disease point prevalence was 3.2 cases per 1,000 children in August 2013. Establishment of a coordinated acute rheumatic fever and rheumatic heart disease control program in American Samoa, likely would improve diagnosis, treatment, and patient compliance with BPG prophylaxis.
急性风湿热是A组链球菌性咽炎(链球菌性喉炎)的一种非化脓性、免疫介导的后果。复发性或严重的急性风湿热可导致永久性心脏瓣膜损害和风湿性心脏病,从而增加患心脏疾病(如感染性心内膜炎、中风和充血性心力衰竭)的风险。如果在症状出现后不超过9天内使用抗生素,可预防急性风湿热。长期注射苄星青霉素G(BPG)可有效预防复发性急性风湿热发作,对于确诊为急性风湿热的儿童,建议每3 - 4周注射一次,持续10年或至21岁。2013年8月,针对急性风湿热和风湿性心脏病发病率上升的传闻报告,美国疾病控制与预防中心(CDC)与美属萨摩亚卫生部及林登·B·约翰逊热带医疗中心(美属萨摩亚唯一的医院)合作,对美属萨摩亚小儿急性风湿热和风湿性心脏病的病例数进行量化,并评估咽炎漏诊、缺乏及时的预防用药处方以及对规定的BPG预防措施的依从性的潜在作用。利用病历数据,2011年和2012年,急性风湿热发病率分别为每1000名≤18岁儿童中1.1例和1.5例;急性风湿热患者中有49%随后被诊断为风湿性心脏病。在65例患者中,有22例(34%)在医生诊断为急性风湿热后未按推荐使用BPG进行预防。2013年8月,风湿性心脏病点患病率为每1000名儿童中3.2例。在美属萨摩亚建立一个协调的急性风湿热和风湿性心脏病控制项目,可能会改善诊断、治疗以及患者对BPG预防措施的依从性。