Pichon-Riviere Andrés, Glujovsky Demián, Garay Osvaldo Ulises, Augustovski Federico, Ciapponi Agustin, Serpa Magdalena, Althabe Fernando
Department of Health Technology Assessment and Economic Evaluation, Institute for Clinical Effectiveness and Health Policy (IECS). Buenos Aires, Argentina.
Maternal and Child Health Integrated-Program (MCHIP)-PATH, Washington, D. C., United States of America.
PLoS One. 2015 Jun 9;10(6):e0129044. doi: 10.1371/journal.pone.0129044. eCollection 2015.
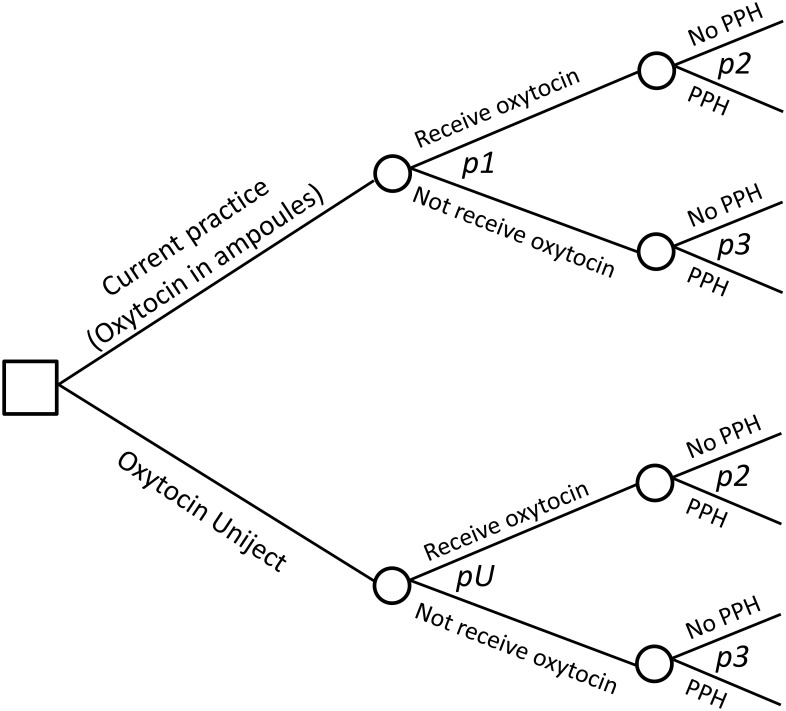
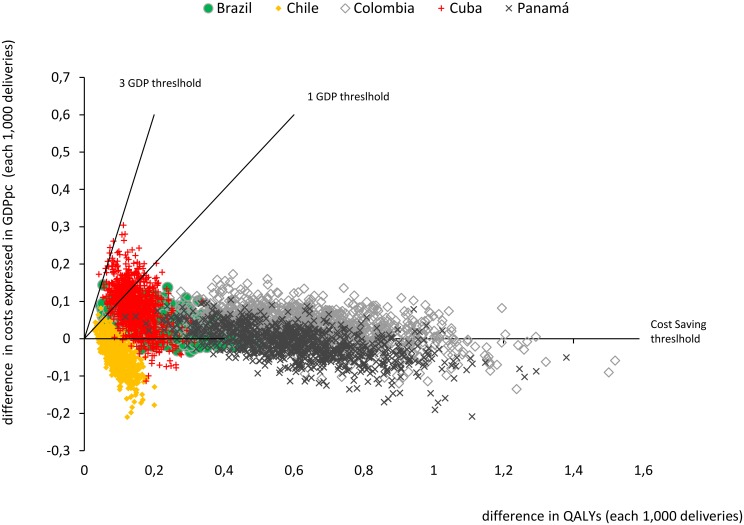
Postpartum hemorrhage (PPH) is a leading cause of maternal death. Despite strong evidence showing the efficacy of routine oxytocin in preventing PPH, the proportion of women receiving it after delivery is still below 100%. The Uniject injection system prefilled with oxytocin (Uniject) has the potential advantage, due to its ease of use, to increase oxytocin utilization rates. We aimed to assess its cost-effectiveness in Latin America and the Caribbean (LAC). We used an epidemiological model to estimate: a) the impact of replacing oxytocin in ampoules with Uniject on the incidence of PPH, quality-adjusted life years (QALYs) and costs from a health care system perspective, and b) the minimum increment in oxytocin utilization rates required to make Uniject a cost-effective strategy. A consensus panel of LAC experts was convened to quantify the expected increase in oxytocin rates as a consequence of making Uniject available. Deterministic and probabilistic sensitivity analyses were performed. In the base case, the incremental cost of Uniject with respect to oxytocin in ampoules was estimated to be USD 1.00 (2013 US dollars). In the cost-effectiveness analysis, Uniject ranged from being cost-saving (in 8 out of 30 countries) to having an incremental cost-effectiveness ratio (ICER) of USD 8,990 per QALY gained. In most countries these ICERs were below one GDP per capita. The minimum required increment in oxytocin rates to make Uniject a cost-effective strategy ranged from 1.3% in Suriname to 16.2% in Haiti. Switching to Uniject could prevent more than 40,000 PPH events annually in LAC. Uniject was cost-saving or very cost-effective in almost all countries. Even if countries can achieve only small increases in oxytocin rates by incorporating Uniject, this strategy could be considered a highly efficient use of resources. These results were robust in the sensitivity analysis under a wide range of assumptions.
产后出血(PPH)是孕产妇死亡的主要原因。尽管有强有力的证据表明常规使用缩宫素预防产后出血有效,但产后接受缩宫素治疗的女性比例仍低于100%。预装缩宫素的一次性注射系统(Uniject)因其使用方便,具有提高缩宫素利用率的潜在优势。我们旨在评估其在拉丁美洲和加勒比地区(LAC)的成本效益。我们使用了一个流行病学模型来估计:a)从医疗保健系统的角度来看,用Uniject替代安瓿装缩宫素对产后出血发生率、质量调整生命年(QALYs)和成本的影响;b)使Uniject成为具有成本效益策略所需的缩宫素利用率的最小增幅。召集了一个拉丁美洲和加勒比地区专家共识小组,以量化因提供Uniject而导致的缩宫素使用率的预期增加。进行了确定性和概率性敏感性分析。在基础案例中,与安瓿装缩宫素相比,Uniject的增量成本估计为1.00美元(2013年美元)。在成本效益分析中,Uniject的范围从节省成本(30个国家中的8个)到每获得一个QALY的增量成本效益比(ICER)为8990美元。在大多数国家,这些ICER低于人均国内生产总值。使Uniject成为具有成本效益策略所需的缩宫素使用率的最小增幅范围从苏里南的1.3%到海地的16.2%。改用Uniject每年可在拉丁美洲和加勒比地区预防超过40000例产后出血事件。在几乎所有国家,Uniject都是节省成本或极具成本效益的。即使各国通过采用Uniject仅能使缩宫素使用率实现小幅提高,该策略也可被视为资源的高效利用。在广泛假设下的敏感性分析中,这些结果是稳健的。