Nephrology and Urology Clinical Institute (ICNU), Hospital Clinic, University of Barcelona, Barcelona, Spain and Hospital Clinic, Institut d'investigacions Biomèdiques August Pi i Suñer (IDIBAPS), University of Barcelona, Barcelona, Spain.
Clin Kidney J. 2012 Feb;5(1):28-30. doi: 10.1093/ndtplus/sfr107. Epub 2012 Jan 28.
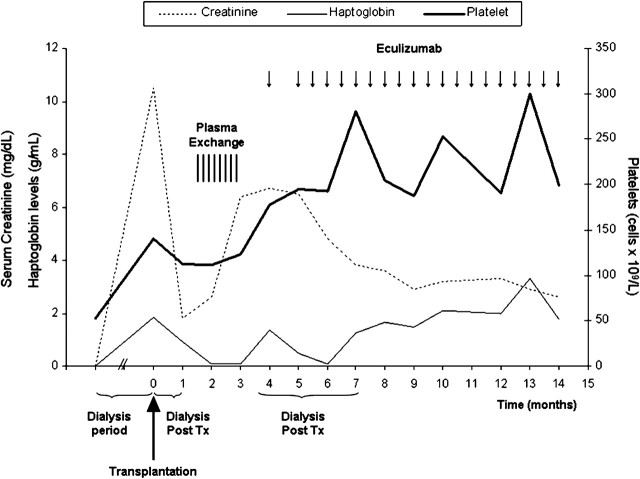
Haemolytic-uraemic syndrome is a clinical syndrome characterized by thrombocytopaenia, non-autoimmune haemolytic anaemia and renal impairment. Pathological alterations in kidney samples show thrombotic microangiopathy. The underlying pathogenesis is endothelial cell injury with thrombotic occlusion of the arterioles and capillaries. A variety of causes have been identified, associated with infection of Escherichia coli O157:H7, environmental factors as immunosuppressive drugs and genetic deficiencies in complement regulatory factors. The latter is called atypical haemolytic-uraemic syndrome (aHUS). Here, we present a patient with severe aHUS with complement factor H deficiency triggered by cocaine use and recurrence after kidney transplantation. The patient restarted haemodialysis for severe renal insufficiency and anti-C5 antibody eculizumab was used as salvage treatment with progressive recovery of graft function and suppression of dialysis.
溶血尿毒综合征是一种以血小板减少、非自身免疫性溶血性贫血和肾功能损害为特征的临床综合征。肾脏样本的病理改变表现为血栓性微血管病。其潜在的发病机制是内皮细胞损伤,伴有小动脉和毛细血管的血栓闭塞。已经确定了多种病因,与大肠杆菌 O157:H7 感染、免疫抑制剂等环境因素以及补体调节因子的遗传缺陷有关。后者称为非典型溶血尿毒综合征(aHUS)。在这里,我们介绍了一例由可卡因使用引发的严重 aHUS 患者,该患者存在补体因子 H 缺乏,且在肾移植后复发。该患者因严重肾功能不全重新开始血液透析,并用抗 C5 抗体依库珠单抗进行挽救性治疗,移植肾功能逐渐恢复,透析得以抑制。