Snow Robert W, Kibuchi Eliud, Karuri Stella W, Sang Gilbert, Gitonga Caroline W, Mwandawiro Charles, Bejon Philip, Noor Abdisalan M
Spatial Health Metrics Group, Kenya Medical Research Institute-Wellcome Trust Research Programme, Nairobi, Kenya; Centre for Tropical Medicine & Global Health, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, United Kingdom.
Spatial Health Metrics Group, Kenya Medical Research Institute-Wellcome Trust Research Programme, Nairobi, Kenya.
PLoS One. 2015 Jun 24;10(6):e0128792. doi: 10.1371/journal.pone.0128792. eCollection 2015.
Progress toward reducing the malaria burden in Africa has been measured, or modeled, using datasets with relatively short time-windows. These restricted temporal analyses may miss the wider context of longer-term cycles of malaria risk and hence may lead to incorrect inferences regarding the impact of intervention.
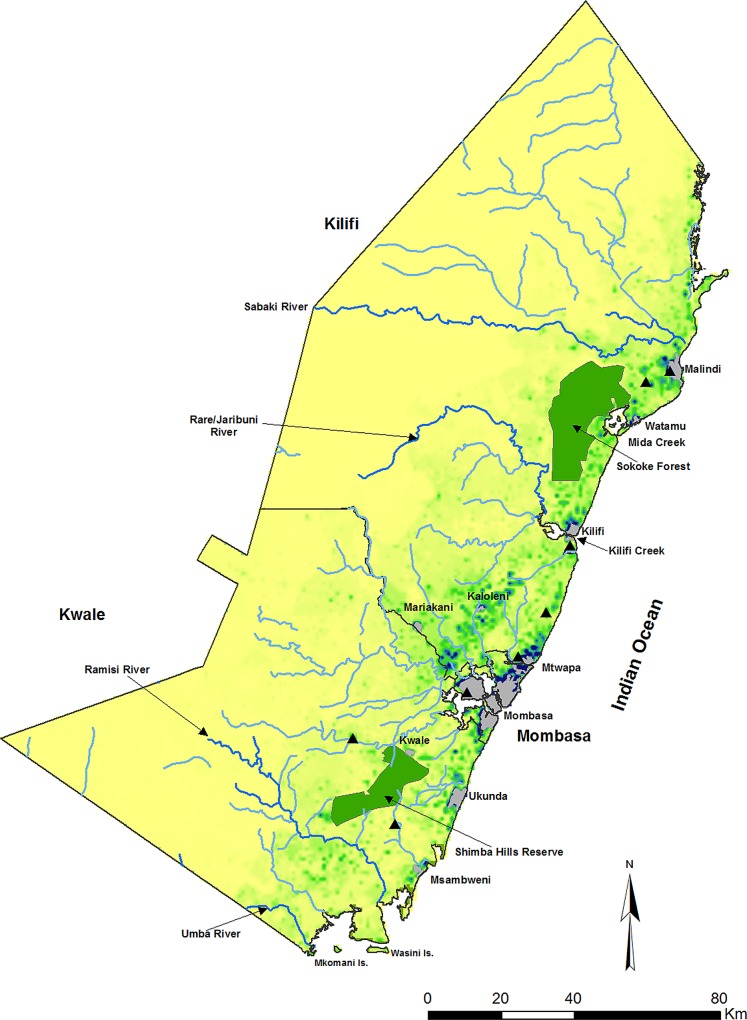
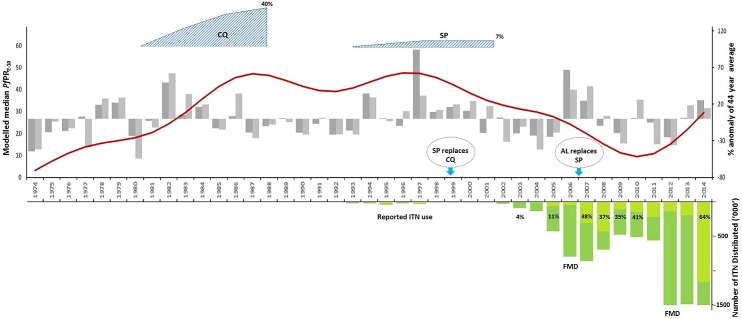
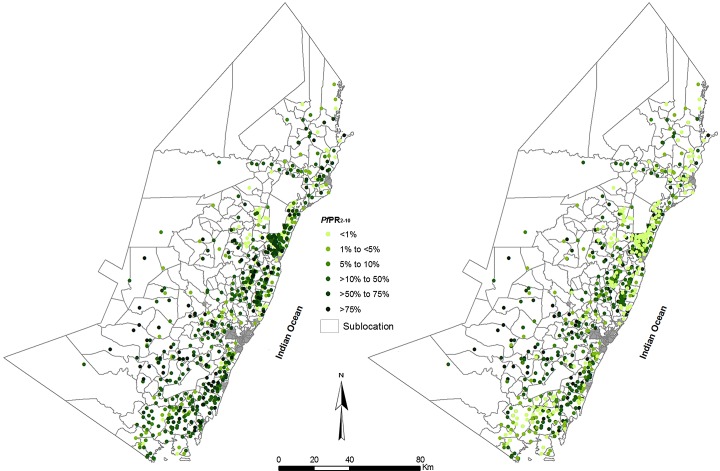
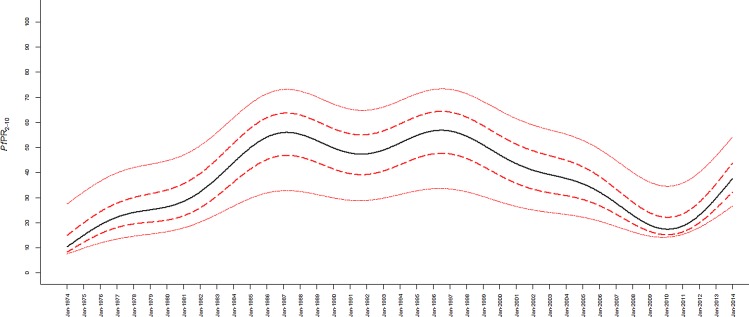
1147 age-corrected Plasmodium falciparum parasite prevalence (PfPR2-10) surveys among rural communities along the Kenyan coast were assembled from 1974 to 2014. A Bayesian conditional autoregressive generalized linear mixed model was used to interpolate to 279 small areas for each of the 41 years since 1974. Best-fit polynomial splined curves of changing PfPR2-10 were compared to a sequence of plausible explanatory variables related to rainfall, drug resistance and insecticide-treated bed net (ITN) use.
P. falciparum parasite prevalence initially rose from 1974 to 1987, dipped in 1991-92 but remained high until 1998. From 1998 onwards prevalence began to decline until 2011, then began to rise through to 2014. This major decline occurred before ITNs were widely distributed and variation in rainfall coincided with some, but not all, short-term transmission cycles. Emerging resistance to chloroquine and introduction of sulfadoxine/pyrimethamine provided plausible explanations for the rise and fall of malaria transmission along the Kenyan coast.
Progress towards elimination might not be as predictable as we would like, where natural and extrinsic cycles of transmission confound evaluations of the effect of interventions. Deciding where a country lies on an elimination pathway requires careful empiric observation of the long-term epidemiology of malaria transmission.
非洲在减轻疟疾负担方面所取得的进展,一直是通过相对较短时间窗口的数据集进行衡量或建模的。这些受限的时间分析可能会忽略疟疾风险长期周期的更广泛背景,因此可能导致对干预措施影响的错误推断。
收集了1974年至2014年间肯尼亚沿海农村社区1147次年龄校正后的恶性疟原虫寄生虫流行率(PfPR2-10)调查数据。使用贝叶斯条件自回归广义线性混合模型对1974年以来41年中的每一年的279个小区域进行插值。将不断变化的PfPR2-10的最佳拟合多项式样条曲线与一系列与降雨、耐药性和经杀虫剂处理的蚊帐(ITN)使用相关的合理解释变量进行比较。
恶性疟原虫寄生虫流行率最初在1974年至1987年上升,在1991 - 1992年下降,但直到1998年一直保持在高位。从1998年起流行率开始下降直到2011年,然后在2014年之前开始上升。这一主要下降发生在ITN广泛分发之前,降雨变化与一些但并非所有短期传播周期相吻合。对氯喹出现的耐药性以及磺胺多辛/乙胺嘧啶的引入,为肯尼亚沿海疟疾传播的起伏提供了合理的解释。
在消除疟疾方面取得的进展可能不像我们期望的那样可预测,因为自然和外部传播周期会混淆对干预措施效果的评估。确定一个国家在消除疟疾道路上所处的位置,需要对疟疾传播的长期流行病学进行仔细的实证观察。