Kumar B Siddhartha, Ravisankar A, Mohan Alladi, Kumar D Prabath, Katyarmal D T, Sachan Alok, Sarma K V S
Division of Rheumatology, Department of Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati, India.
Indian J Med Res. 2015 Apr;141(4):431-7. doi: 10.4103/0971-5916.159287.
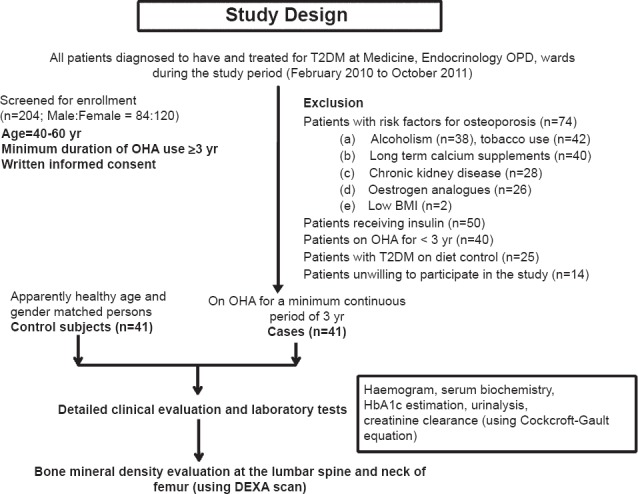
BACKGROUND & OBJECTIVES: Type 2 diabetes mellitus (T2DM) is considered to be a protective factor against development of osteoporosis. But oral hypoglycaemic agents (OHA) are likely to increase the risk of osteoporosis. This study was carried out to evaluate the effect of various OHA on bone mineral density (BMD) in patients with T2DM.
Forty one patients (study group) with T2DM (mean age 51.9±5.5 yr; 31 females) receiving treatment with oral hypoglycaemic agents (OHA) [thiazolidinediones alone (n=14) or in combination with other OHA (n=27)] for a period of at least three consecutive years and 41 age- and gender-matched healthy controls (mean age 51.4±5.1 yr) were included in the study. A detailed clinical history was taken and all were subjected to physical examination and recording of anthropometric data. BMD was assessed for both patients and controls.
The mean body mass index (kg/m [2] ) (26.5±4.90 vs 27.3 ±5.33) and median [inter-quartile range (IQR)] duration of menopause (yr) among women [6(2-12) vs 6(1-13)] were comparable between both groups. The bone mineral density (BMD; g/cm [2] ) at the level of neck of femur (NOF) (0.761±0.112 vs 0.762±0.110), lumbar spine antero-posterior view (LSAP) (0.849±0.127 vs 0.854±0.135); median Z-score NOF {0.100[(-0.850)-(0.550)] vs -0.200[(-0.800)-(0.600)]}, LSAP {-1.200[(-1.700)-(-0.200)] vs -1.300 [(-1.85)-(-0.400)]} were also similar in study and control groups. Presence of normal BMD (9/41 vs 8/41), osteopenia (16/41 vs 18/41) and osteoporosis (16/41 vs 15/41) were comparable between the study and control groups. No significant difference was observed in the BMD, T-scores and Z-scores at NOF and LSAP among T2DM patients treated with thiazolidinediones; those treated with other OHA and controls.
INTERPRETATION & CONCLUSIONS: The present findings show that the use of OHA for a period of three years or more does not significantly affect the BMD in patients with T2DM.
2型糖尿病(T2DM)被认为是预防骨质疏松症发生的一个保护因素。但口服降糖药(OHA)可能会增加骨质疏松症的风险。本研究旨在评估各种OHA对T2DM患者骨密度(BMD)的影响。
41例接受口服降糖药(OHA)治疗(单独使用噻唑烷二酮类药物治疗的患者14例,联合其他OHA治疗的患者27例)至少连续三年的T2DM患者(研究组),平均年龄51.9±5.5岁,其中女性31例,以及41例年龄和性别匹配的健康对照者(平均年龄51.4±5.1岁)纳入本研究。详细记录临床病史,所有受试者均进行体格检查并记录人体测量数据。对患者和对照者均进行骨密度评估。
两组间平均体重指数(kg/m²)(26.5±4.90 vs 27.3±5.33)以及女性绝经时间中位数[四分位数间距(IQR),年] [6(2 - 12)vs 6(1 - 13)]相当。股骨颈(NOF)水平骨密度(BMD,g/cm²)(0.761±0.112 vs 0.762±0.110)、腰椎前后位(LSAP)(0.849±0.127 vs 0.854±0.135);NOF的Z值中位数{0.100[(-0.850)-(0.550)] vs -0.200[(-0.800)-(0.600)]}、LSAP {-1.200[(-1.700)-(-0.200)] vs -1.300 [(-1.85)-(-0.400)]}在研究组和对照组中也相似。骨密度正常者(9/41 vs 8/41)、骨量减少者(16/41 vs 18/41)和骨质疏松者(16/41 vs 15/41)在研究组和对照组中的比例相当。在接受噻唑烷二酮类药物治疗的T2DM患者、接受其他OHA治疗的患者以及对照组之间,NOF和LSAP处的BMD、T值和Z值均未观察到显著差异。
目前的研究结果表明,使用OHA三年或更长时间对T2DM患者的骨密度没有显著影响。