Salem Katayoun, Khoshrang Hossein, Kousha Maryam, Hoseini Mahboobeh, Ranjbar Marzieh, Baniasadi Shadi, Salamzadeh Jamshid
Department of Pediatric Dentistry and Dentistry Hospital, Guilan Dental School, Rasht, IR Iran.
Department of Anesthesiology, Guilan University of Medical Sciences, Rasht, IR Iran.
Iran J Pediatr. 2015 Jun;25(3):e494. doi: 10.5812/ijp.25(3)2015.494. Epub 2015 Jun 27.
Among different categories of sedative agents, benzodiazepines have been prescribed for more than three decades to patients of all ages. The effective and predictable sedative and amnestic effects of benzodiazepines support their use in pediatric patients. Midazolam is one of the most extensively used benzodiazepines in this age group. Oral form of drug is the best accepted route of administration in children.
The purpose of this study was to compare the efficacy and safety of a commercially midazolam syrup versus orally administered IV midazolam in uncooperative dental patients. Second objective was to determine whether differences concerning sedation success can be explained by child's behavioral problems and dental fear.
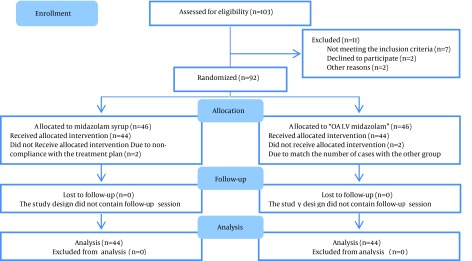
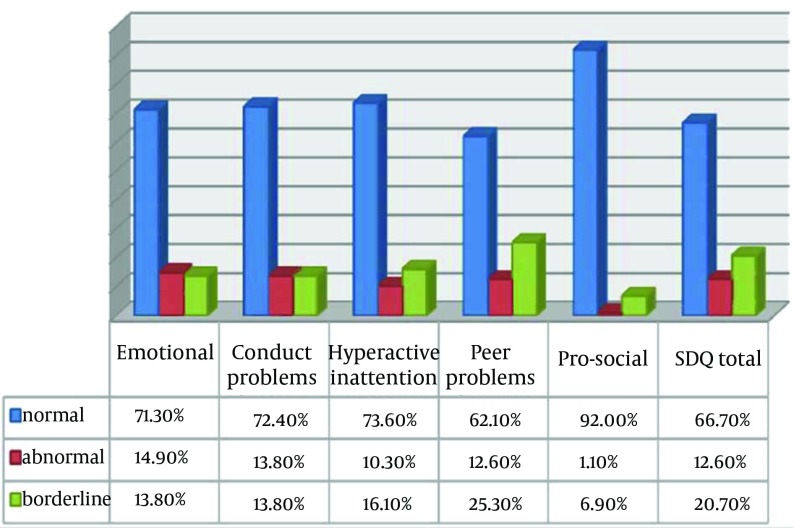
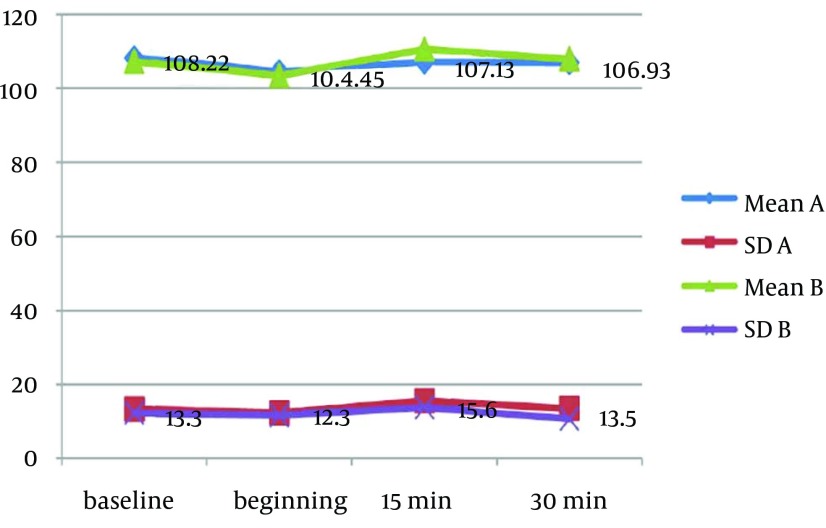
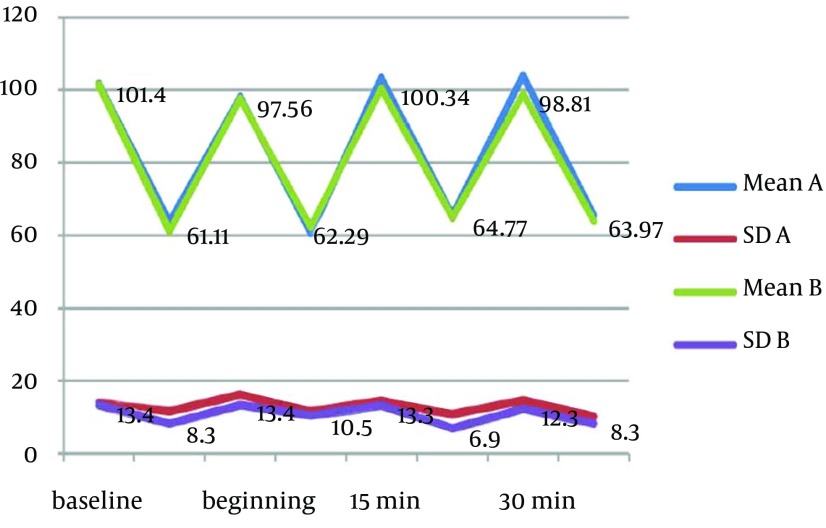
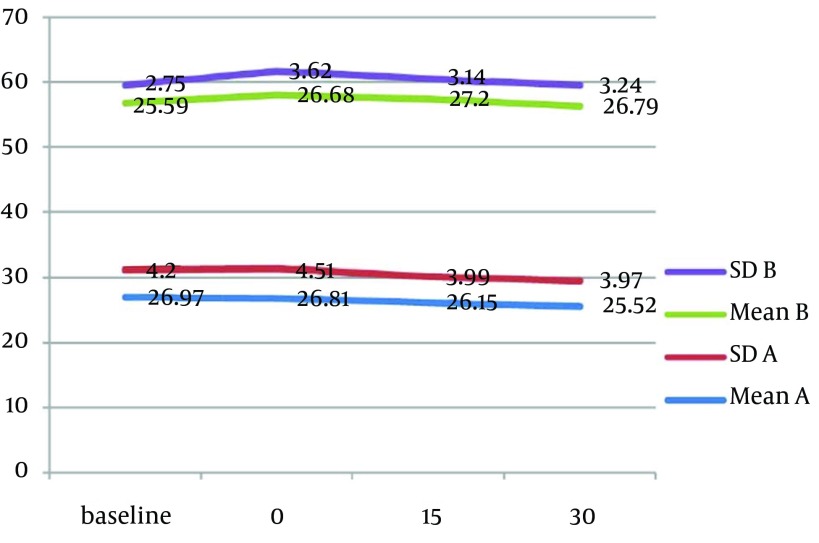
Eighty eight uncooperative dental patients (Frankl Scales 1,2) aged 3 to 6 years, and ASA I participated in this double blind, parallel randomized, controlled clinical trial. Midazolam was administered in a dose of 0.5 mg/kg for children under the age 5 and 0.2 mg/kg in patients over 5 years of age. Physiologic parameters including heart rate, respiratory rate, oxygen saturation and blood pressure were recorded. Behavior assessment was conducted throughout the course of treatment using Houpt Sedation Rating Scale and at critical moments of treatment (injection and cavity preparation) by North Carolina Scale. Dental fear and behavioral problems were evaluated using Child Fear Schedule Survey-Dental Subscale (CFSS-DS), and Strength and Difficulties Questionnaire (SDQ). Independent t-test, Chi-Square, and Pearson correlation were used for statistical analysis.
Acceptable overall sedation ratings were observed in 90% and 86% of syrup and IV/Oral group respectively; Chi-Square P = 0.5. Other domains of Houpt Scale including: sleep, crying and movement were also not significantly different between groups. Physiological parameters remained in normal limits during study without significant difference between groups.
"Orally administered IV midazolam" preparation can be used as an alternative for commercially midazolam syrup.
在不同种类的镇静剂中,苯二氮䓬类药物已被处方给各年龄段患者超过三十年。苯二氮䓬类药物有效且可预测的镇静和遗忘作用支持其在儿科患者中的使用。咪达唑仑是该年龄组中使用最广泛的苯二氮䓬类药物之一。药物的口服剂型是儿童最易接受的给药途径。
本研究的目的是比较市售咪达唑仑糖浆与口服静脉注射咪达唑仑在不合作牙科患者中的疗效和安全性。第二个目的是确定镇静成功率的差异是否可以由儿童的行为问题和牙科恐惧来解释。
八十八名年龄在3至6岁、美国麻醉医师协会(ASA)分级为I级的不合作牙科患者参与了这项双盲、平行随机对照临床试验。5岁以下儿童咪达唑仑的给药剂量为0.5mg/kg,5岁以上患者为0.2mg/kg。记录包括心率、呼吸频率、血氧饱和度和血压在内的生理参数。在整个治疗过程中使用豪普特镇静评分量表进行行为评估,并在治疗的关键时刻(注射和窝洞制备)使用北卡罗来纳量表进行评估。使用儿童恐惧量表调查 - 牙科分量表(CFSS - DS)和长处与困难问卷(SDQ)评估牙科恐惧和行为问题。采用独立t检验、卡方检验和皮尔逊相关性分析进行统计分析。
糖浆组和静脉注射/口服组分别有90%和86%的患者获得了可接受的总体镇静评分;卡方检验P = 0.5。豪普特量表的其他领域,包括:睡眠、哭闹和活动,两组之间也无显著差异。研究期间生理参数保持在正常范围内,两组之间无显著差异。
“口服静脉注射咪达唑仑”制剂可作为市售咪达唑仑糖浆的替代品。