Reant Patricia, Captur Gabriella, Mirabel Mariana, Nasis Arthur, M Sado Daniel, Maestrini Viviana, Castelletti Silvia, Manisty Charlotte, Herrey Anna S, Syrris Petros, Tome-Esteban Maite, Jenkins Sharon, Elliott Perry M, McKenna William J, Moon James C
Division of Cardiovascular Imaging and Inherited Cardiac Disease Unit, The Heart Hospital, Institute of Cardiovascular Science, University College London, London, UK.
Hôpital Cardiologique du Haut-Levêque (Pessac), CHU de Bordeaux, Université de Bordeaux, Bordeaux, France.
J Cardiovasc Magn Reson. 2015 Jul 30;17(1):64. doi: 10.1186/s12968-015-0160-y.
Sarcomeric gene mutations cause hypertrophic cardiomyopathy (HCM). In gene mutation carriers without left ventricular (LV) hypertrophy (G + LVH-), subclinical imaging biomarkers are recognized as predictors of overt HCM, consisting of anterior mitral valve leaflet elongation, myocardial crypts, hyperdynamic LV ejection fraction, and abnormal apical trabeculation. Reverse curvature of the interventricular septum (into the LV) is characteristic of overt HCM. We aimed to assess LV septal convexity in subclinical HCM.
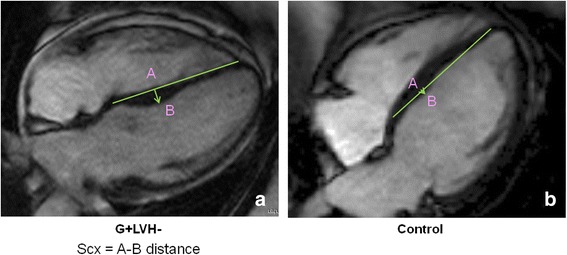
Cardiovascular magnetic resonance was performed on 36 G + LVH- individuals (31 ± 14 years, 33 % males) with a pathogenic sarcomere mutation, and 36 sex and age-matched healthy controls (33 ± 12 years, 33 % males). Septal convexity (SCx) was measured in the apical four chamber view perpendicular to a reference line connecting the mid-septal wall at tricuspid valve insertion level and the apical right ventricular insertion point.
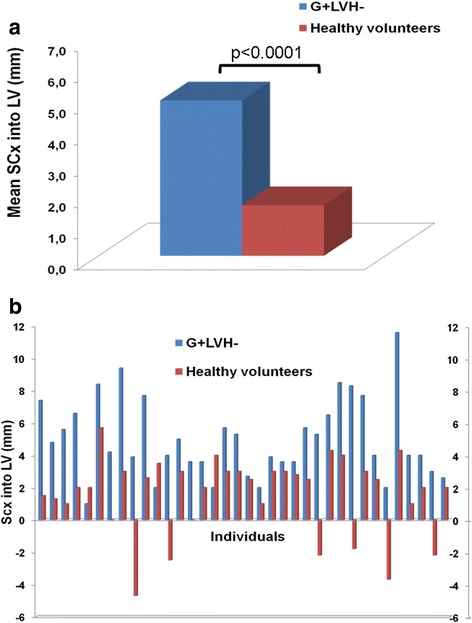
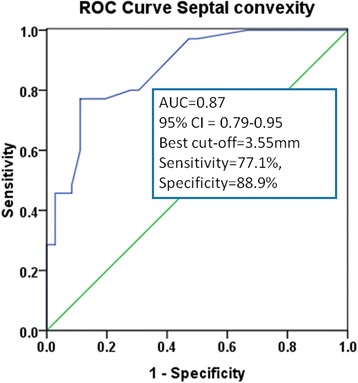
Septal convexity was increased in G + LVH- compared to controls (maximal distance of endocardium to reference line: 5.0 ± 2.5 mm vs. 1.6 ± 2.4 mm, p ≤ 0.0001). Expected findings occurred in G + LVH- individuals: longer anterior mitral valve leaflet (23.5 ± 3.0 mm vs. 19.9 ± 3.1 mm, p ≤ 0.0001), higher relative wall thickness (0.31 ± 0.05 vs. 0.29 ± 0.04, p ≤ 0.05), higher LV ejection fraction (70.8 ± 4.3 % vs. 68.3 ± 4.4 %, p ≤ 0.05), and smaller LV end-systolic volume index (21.4 ± 4.4 ml/m(2) vs. 23.7 ± 5.8 ml/m(2), p ≤ 0.05). Other morphologic measurements (LV angles, sphericity index, and eccentricity index) were not different between G + LVH- and controls.
Septal convexity is an additional previously undescribed feature of subclinical HCM.
肌节基因突变可导致肥厚型心肌病(HCM)。在无左心室(LV)肥厚的基因突变携带者(G+LVH-)中,亚临床影像生物标志物被认为是显性HCM的预测指标,包括二尖瓣前叶延长、心肌隐窝、左室射血分数增高及心尖小梁异常。室间隔向LV内反向弯曲是显性HCM的特征。我们旨在评估亚临床HCM中的左室间隔凸度。
对36例携带致病性肌节基因突变的G+LVH-个体(31±14岁,33%为男性)和36例年龄及性别匹配的健康对照者(33±12岁,33%为男性)进行心血管磁共振检查。在垂直于连接三尖瓣附着水平室间隔壁中点与心尖右室附着点的参考线的心尖四腔视图中测量间隔凸度(SCx)。
与对照组相比,G+LVH-个体的间隔凸度增加(心内膜到参考线的最大距离:5.0±2.5mm对1.6±2.4mm,p≤0.0001)。G+LVH-个体出现了预期的表现:二尖瓣前叶更长(23.5±3.0mm对19.9±3.1mm,p≤0.0001)、相对室壁厚度更高(0.31±0.05对0.29±0.04,p≤0.05)、左室射血分数更高(70.8±4.3%对68.3±4.4%,p≤0.05)以及左室收缩末期容积指数更小(21.4±4.4ml/m²对23.7±5.8ml/m²,p≤0.05)。G+LVH-个体与对照组之间的其他形态学测量指标(左室角度、球形指数和偏心指数)无差异。
间隔凸度是亚临床HCM另一个先前未描述的特征。