Beck Marcus, Ghadjar Pirus, Weihrauch Mirko, Burock Susen, Budach Volker, Nadobny Jacek, Sehouli Jalid, Wust Peter
Department of Radiation Oncology, Charité Universitätsmedizin Berlin, Augustenburger Platz 1, 13353, Berlin, Germany.
Charité Comprehensive Cancer Center, Charité Universitätsmedizin Berlin, Berlin, Germany.
Radiat Oncol. 2015 Jul 30;10:157. doi: 10.1186/s13014-015-0451-3.
Peritoneal carcinomatosis occurs in different cancer subtypes and is associated with a dismal prognosis. Some doubts remain whether the whole abdomen can be treated by regional hyperthermia, therefore we analyzed feasibility conducting a pilot study.
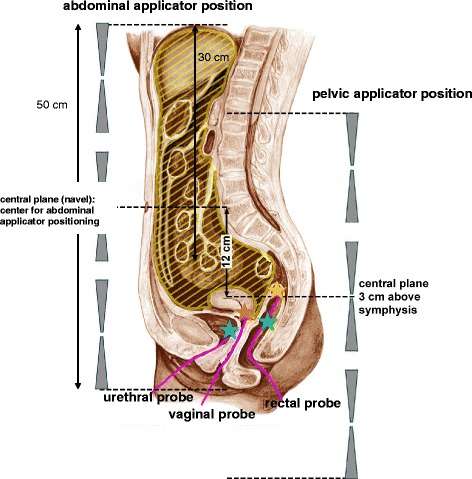
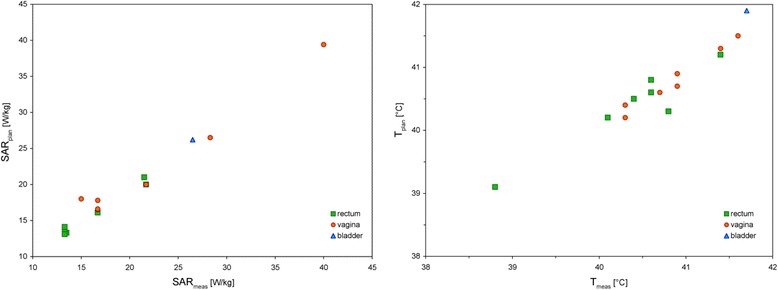
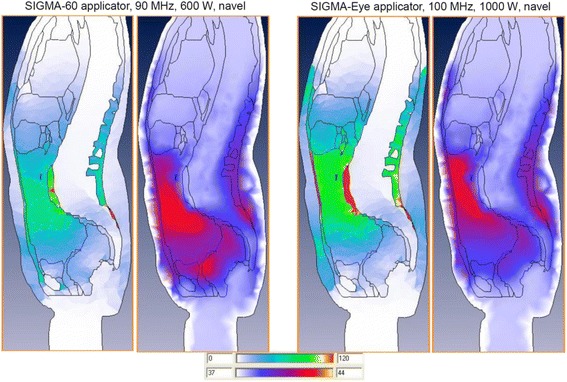
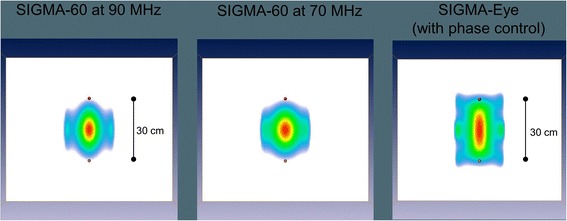
A simulation of the abdominopelvic heat distribution in 11 patients with peritoneal carcinomatosis was done using the HyperPlan software and the SIGMA-60 and SIGMA-Eye applicators. Tissue-specific region-related electrical and thermal parameters were used to solve the Maxwell's equations and the bioheat-transfer equation. Three-dimensional specific absorption rate (SAR) distributions and, additionally, estimated region-related perfusion rates were used to solve the bioheat-transfer equation. The predicted SAR and temperature distributions were compared with minimally invasive measurements in pelvic reference points.
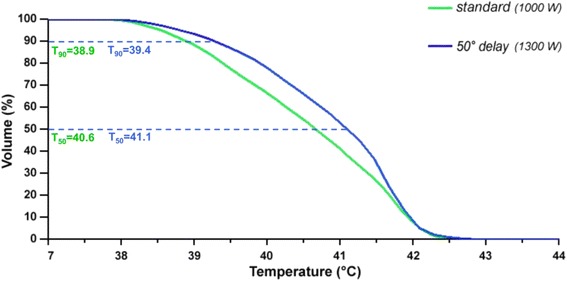
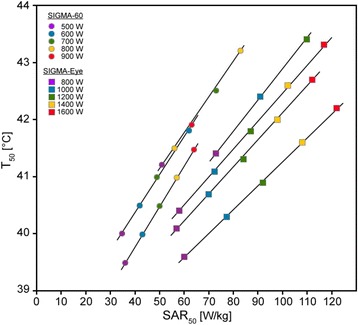
In 11 patients (7 of them treated in the SIGMA-60 and 4 in the SIGMA-Eye applicator) the measured treatment variables (SAR, temperatures in the pelvic reference points) indicated that the heated volumes were higher for the SIGMA-Eye applicator. The mean computed abdominal SARs were less for the SIGMA-Eye (33 versus 44 W/kg). Nevertheless, the temperature distributions in the abdomen (peritoneal cavity) were more homogeneous in the SIGMA-Eye applicator as compared to the SIGMA-60 as indicated by higher values of T90 (mean 40.2 versus 38.2 °C) and T50 (mean 41.1 versus 40.2 °C), while the maximum temperatures were similar (in the range 41 to 43 °C). Even though the mean abdominal SAR was lower in the SIGMA-Eye, the heat distribution covered a larger volume of the abdomen (in particular the upper abdomen). For the SIGMA-60 applicator the achieved T90 appeared to be limited between 41 and 42 °C, for the SIGMA Eye applicator more effective T90 in the range 42 to 43 °C were obtained.
Our results suggest that an adequate heating of the abdomen and therefore abdominal regional hyperthermia in PC patients appears feasible. The SIGMA-Eye applicator appears to be superior compared to the SIGMA-60 applicator for abdominal hyperthermia.
腹膜癌病发生于不同的癌症亚型,预后较差。对于全腹是否可用区域热疗进行治疗仍存在一些疑问,因此我们开展了一项初步研究以分析其可行性。
使用HyperPlan软件以及SIGMA - 60和SIGMA - Eye施源器对11例腹膜癌病患者的腹盆腔热分布进行模拟。采用组织特异性区域相关的电学和热学参数求解麦克斯韦方程和生物热传递方程。利用三维比吸收率(SAR)分布以及估计的区域相关灌注率求解生物热传递方程。将预测的SAR和温度分布与盆腔参考点的微创测量结果进行比较。
在11例患者中(7例使用SIGMA - 60施源器治疗,4例使用SIGMA - Eye施源器治疗),所测量的治疗变量(SAR、盆腔参考点的温度)表明,SIGMA - Eye施源器的加热体积更大。SIGMA - Eye施源器的平均计算腹部SAR较低(33 W/kg对44 W/kg)。然而,与SIGMA - 60相比,SIGMA - Eye施源器在腹部(腹腔)的温度分布更均匀,T90(平均40.2℃对38.2℃)和T50(平均41.1℃对40.2℃)值更高,而最高温度相似(在41至43℃范围内)。尽管SIGMA - Eye施源器的平均腹部SAR较低,但其热分布覆盖的腹部体积更大(特别是上腹部)。对于SIGMA - 60施源器,所达到的T90似乎限制在41至42℃之间,对于SIGMA Eye施源器,获得了更有效的42至43℃范围内的T90。
我们的结果表明,对腹膜癌病患者的腹部进行充分加热以及因此进行腹部区域热疗似乎是可行的。在腹部热疗方面,SIGMA - Eye施源器似乎优于SIGMA - 60施源器。