Lee Douglas S, Hardy Judy, Yee Raymond, Healey Jeffrey S, Birnie David, Simpson Christopher S, Crystal Eugene, Mangat Iqwal, Nanthakumar Kumaraswamy, Wang Xuesong, Krahn Andrew D, Dorian Paul, Austin Peter C, Tu Jack V
From the Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada (D.S.L., J.H., X.W., P.C.A., J.V.T.); Peter Munk Cardiac Centre (D.S.L., K.N.) and Joint Department of Medical Imaging (D.S.L.), University Health Network (D.S.L., K.N.), Institute for Health Policy, Management and Evaluation (D.S.L., P.C.A., J.V.T.), Division of Cardiology, Department of Medicine, Sunnybrook Health Sciences Centre (E.C., J.V.T.), and Division of Cardiology, Department of Medicine, St. Michael's Hospital (I.M., P.D.), University of Toronto, Toronto, Ontario, Canada; Division of Cardiology, Department of Medicine, London Health Sciences Centre, University of Western Ontario, London, Ontario, Canada (R.Y.); Division of Cardiology, Department of Medicine, Hamilton Health Sciences Centre, McMaster University, Hamilton, Ontario, Canada (J.S.H.); Division of Cardiology, Department of Medicine, University of Ottawa Heart Institute, Ottawa, Ontario, Canada (D.B.); Kingston General Hospital, Queen's University, Kingston, Ontario, Canada (C.S.S.); and Division of Cardiology, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada (A.D.K.).
Circ Heart Fail. 2015 Sep;8(5):927-37. doi: 10.1161/CIRCHEARTFAILURE.115.002414. Epub 2015 Jul 29.
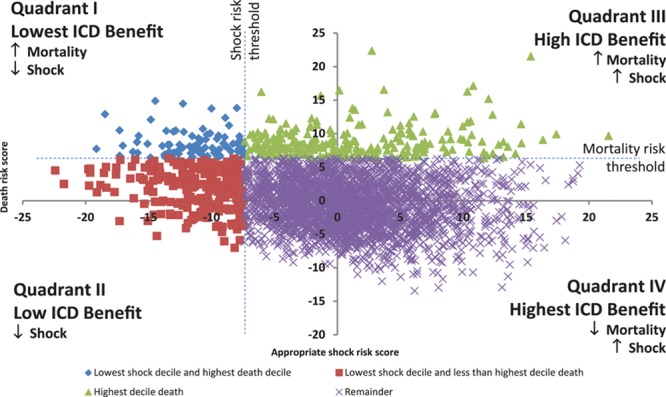
A conceptualized model may be useful for understanding risk stratification of primary prevention implantable cardioverter defibrillators considering the competing risks of appropriate implantable cardioverter defibrillator shock versus mortality.
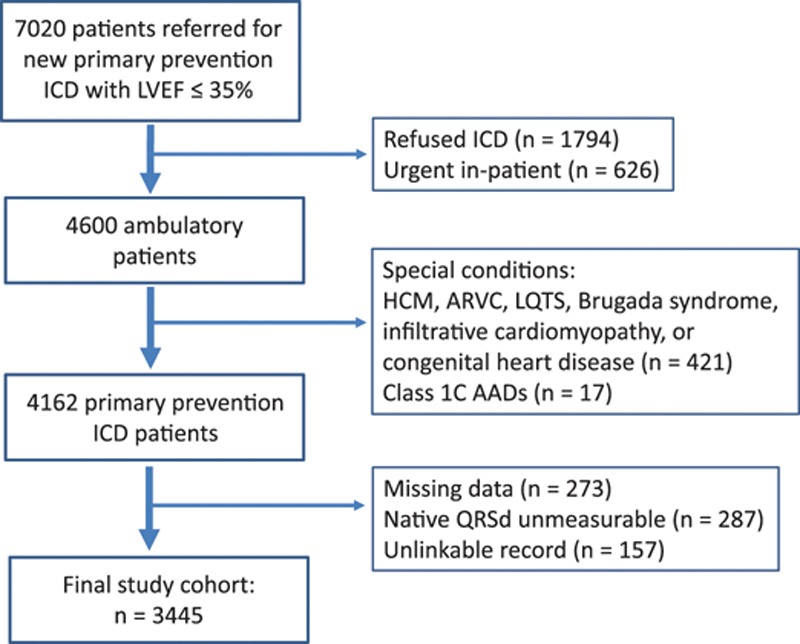
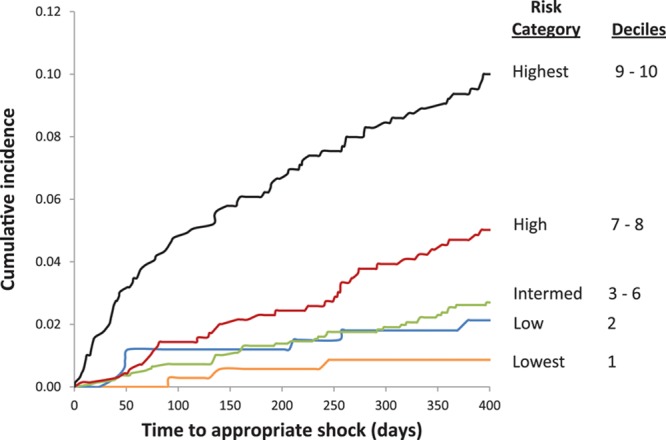
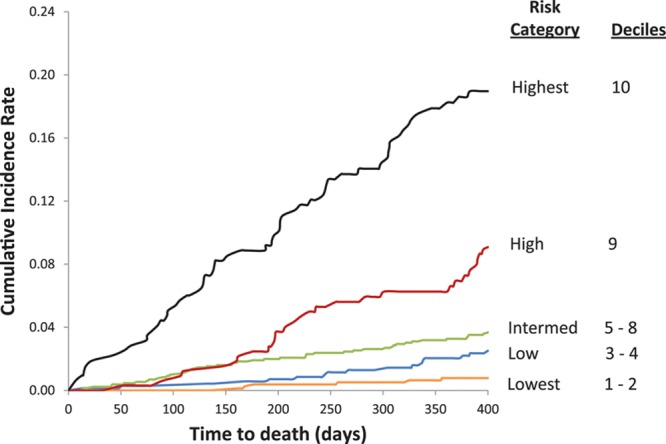
In a prospective, multicenter, population-based cohort with left ventricular ejection fraction ≤35% referred for primary prevention implantable cardioverter defibrillator, we developed dual risk stratification models to determine the competing risks of appropriate defibrillator shock versus mortality using a Fine-Gray subdistribution hazard model. Among 7020 patients referred, 3445 underwent defibrillator implant (79.7% men, median, 66 years [25th, 75th: 58-73]). During 5918 person-years of follow-up, appropriate shock occurred in 204 patients (3.6 shocks/100 person-years) and 292 died (4.9 deaths/100 person-years). Competing risk predictors of appropriate shock included nonsustained ventricular tachycardia, atrial fibrillation, serum creatinine concentration, digoxin or amiodarone use, and QRS duration near 130-ms peak. One-year cumulative incidence of appropriate shock was 0.9% in the lowest risk category, and 1.7%, 2.5%, 4.9%, and 9.3% in low, intermediate, high, and highest risk groups, respectively. Hazard ratios for appropriate shock ranged from 4.04 to 7.79 in the highest 3 deciles (all P≤0.001 versus lowest risk). Cumulative incidence of 1-year death was 0.6%, 1.9%, 3.3%, 6.2%, and 17.7% in lowest, low, intermediate, high, and highest risk groups, respectively. Mortality hazard ratios ranged from 11.48 to 36.22 in the highest 3 deciles (all P<0.001 versus lowest risk).
Simultaneous estimation of risks of appropriate shock and mortality can be performed using clinical variables, providing a potential framework for identification of patients who are unlikely to benefit from prophylactic implantable cardioverter defibrillator.
考虑到恰当的植入式心律转复除颤器(ICD)电击与死亡的竞争风险,一个概念化模型可能有助于理解一级预防植入式心律转复除颤器的风险分层。
在一个前瞻性、多中心、基于人群的队列研究中,纳入左心室射血分数≤35%且因一级预防植入式心律转复除颤器而转诊的患者,我们使用Fine-Gray子分布风险模型开发了双重风险分层模型,以确定恰当的除颤器电击与死亡的竞争风险。在7020名转诊患者中,3445名接受了除颤器植入(男性占79.7%,中位年龄66岁[第25百分位数,第75百分位数:58 - 73岁])。在5918人年的随访期间,204名患者发生了恰当的电击(3.6次电击/100人年),292人死亡(4.9例死亡/100人年)。恰当电击的竞争风险预测因素包括非持续性室性心动过速、心房颤动、血清肌酐浓度、使用地高辛或胺碘酮以及QRS时限接近130毫秒峰值。最低风险类别中恰当电击的1年累积发生率为0.9%,低、中、高和最高风险组分别为1.7%、2.5%、4.9%和9.3%。最高的3个十分位数中恰当电击的风险比范围为4.04至7.79(与最低风险组相比,所有P≤0.001)。最低、低、中、高和最高风险组1年死亡的累积发生率分别为0.6%、1.9%、3.3%、6.2%和17.7%。最高的3个十分位数中死亡风险比范围为11.48至36.22(与最低风险组相比,所有P<0.001)。
使用临床变量可同时估计恰当电击和死亡风险,为识别不太可能从预防性植入式心律转复除颤器中获益的患者提供了一个潜在框架。