Corral Mitra, Ferko Nicole, Hollmann Sarah, Broder Michael S, Chang Eunice
Ethicon Biosurgery, Somerville, NJ, USA.
Cornerstone Research Group, Burlington, ON, Canada.
Clinicoecon Outcomes Res. 2015 Jul 22;7:409-21. doi: 10.2147/CEOR.S86369. eCollection 2015.
Bleeding remains a common occurrence in surgery. Data describing the burden of difficult-to-control bleeding and topical absorbable hemostat use are sparse. This study was conducted to estimate the clinical and economic impact that remains associated with uncontrolled surgical bleeding, even when hemostats are used during surgery.
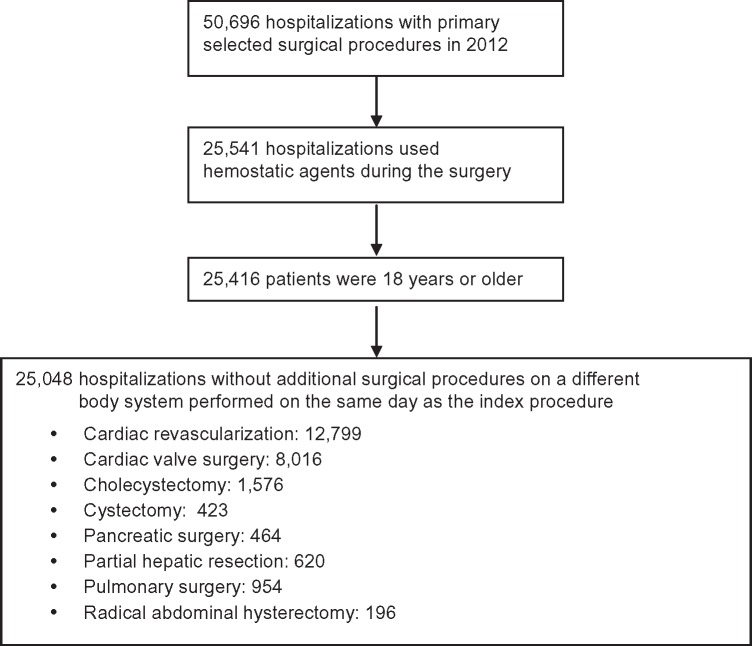
This US retrospective analysis used the Premier Perspectives Database. Hospital discharges from 2012 were used to identify patients treated with hemostats during eight surgery types. Patients were included if they were ≥18 years, had an inpatient hospitalization with one of the eight surgeries, and received a hemostat on the day of surgery. Patients were stratified by procedure and presence or absence of major bleeding (uncontrolled) despite hemostat use. Outcomes were all-cause hospitalization costs, hemostat costs, length of stay, reoperation, and surgery-related complications (eg, mortality). Statistical significance was tested through chi-square or t-tests. Multivariate analyses were conducted for all-cause costs and length of stay using analysis of covariance.
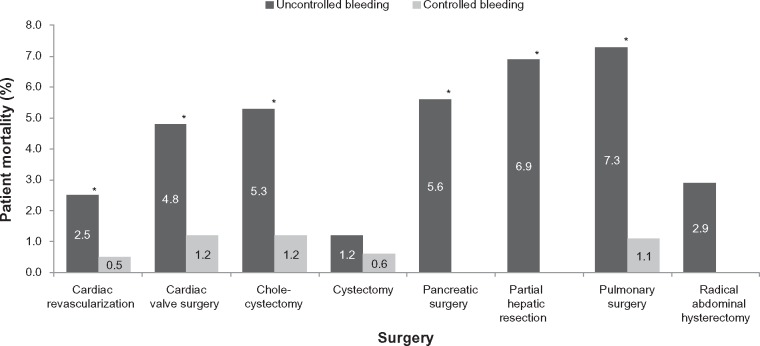
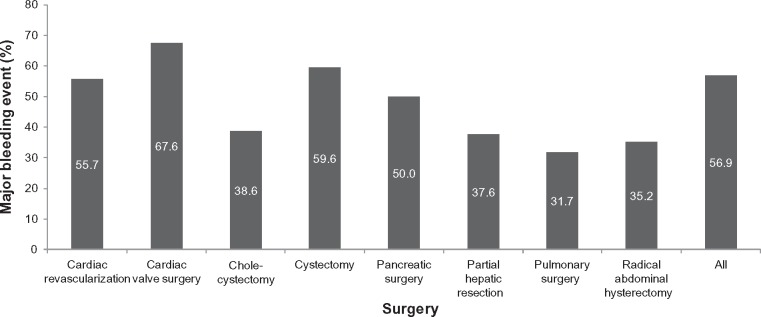
Among 25,048 procedures, major bleeding events occurred in 14,251 cases. Despite treatment with hemostats, major bleeding occurred in 32%-68% of cases. All-cause costs were significantly higher in patients with uncontrolled bleeding despite hemostat use versus controlled bleeding (US$24,203-$61,323 [uncontrolled], US$14,420-$45,593 [controlled]; P<0.001). Hemostat costs were significantly greater in the uncontrolled bleeding cohort for all surgery types except cystectomy and pancreatic surgery. Reoperation and mortality rates were significantly higher in the uncontrolled bleeding cohort in all surgical procedures except cystectomy and radical hysterectomy.
Uncontrolled intraoperative bleeding despite hemostat use is prevalent and associated with significantly higher hospital costs and worse clinical outcomes across several surgical procedures compared to controlled bleeding. There is an unmet need for newer hemostats that can more effectively control bleeding, improve outcomes, and reduce hospital resource use.
出血仍是手术中常见的情况。描述难以控制的出血负担和局部可吸收止血剂使用情况的数据很少。本研究旨在评估即使在手术中使用了止血剂,与未控制的手术出血相关的临床和经济影响。
这项美国回顾性分析使用了Premier Perspectives数据库。利用2012年的医院出院数据来识别接受八种手术类型且使用了止血剂的患者。纳入标准为年龄≥18岁、因八种手术之一住院治疗且在手术当天使用了止血剂的患者。根据手术类型以及使用止血剂后是否发生大出血(未控制)对患者进行分层。观察指标包括全因住院费用、止血剂费用、住院时间、再次手术以及手术相关并发症(如死亡率)。通过卡方检验或t检验进行统计学显著性检验。使用协方差分析对全因费用和住院时间进行多变量分析。
在25048例手术中,14251例发生了大出血事件。尽管使用了止血剂,大出血仍发生在32% - 68%的病例中。使用止血剂后出血未得到控制的患者与出血得到控制的患者相比,全因费用显著更高(未控制组为24203 - 61323美元,控制组为14420 - 45593美元;P<0.001)。除膀胱切除术和胰腺手术外,所有手术类型中出血未得到控制的队列中止血剂费用显著更高。除膀胱切除术和根治性子宫切除术后,所有手术中出血未得到控制的队列再次手术率和死亡率显著更高。
与出血得到控制相比,即使使用了止血剂,术中出血未得到控制的情况仍然普遍存在,并且在多种手术中与显著更高的医院费用和更差的临床结局相关。对于能够更有效控制出血、改善结局并减少医院资源使用的新型止血剂存在未满足的需求。