Rodriguez Annabelle, Magee Michelle, Ramos Pedro, Seley Jane Jeffrie, Nolan Ann, Kulasa Kristen, Caudell Kathryn Ann, Lamb Aimee, MacIndoe John, Maynard Greg
Diabetes Spectr. 2014 Aug;27(3):197-206. doi: 10.2337/diaspect.27.3.197.
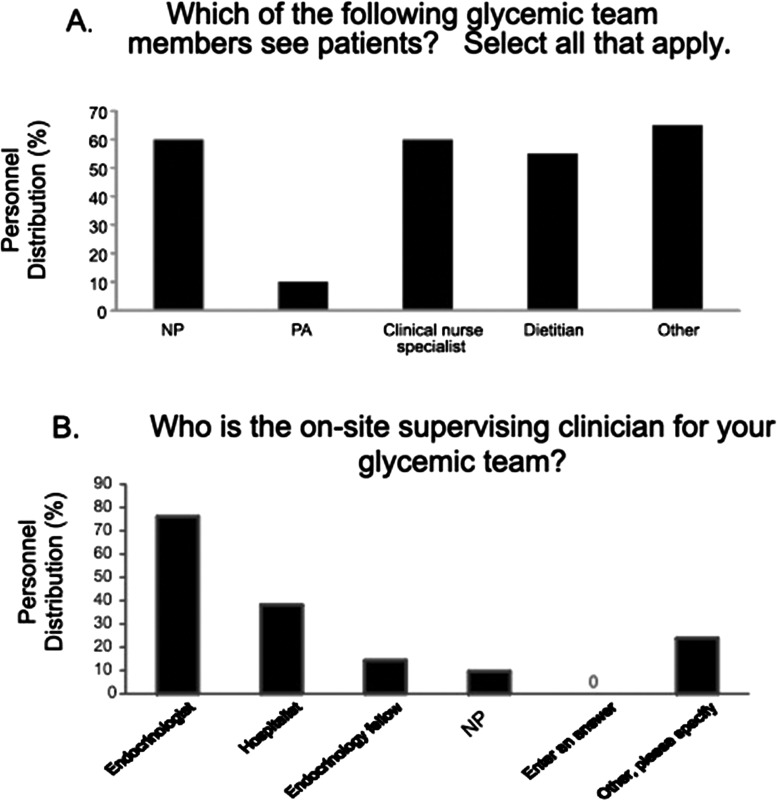
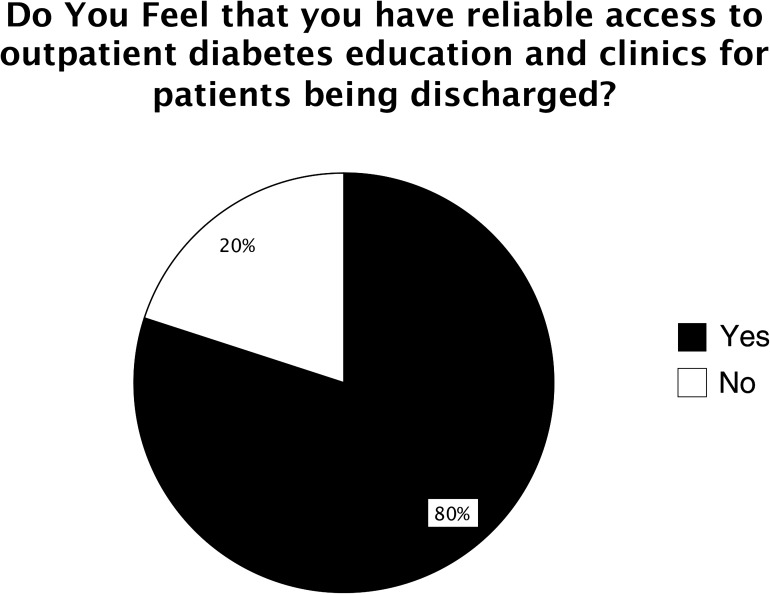
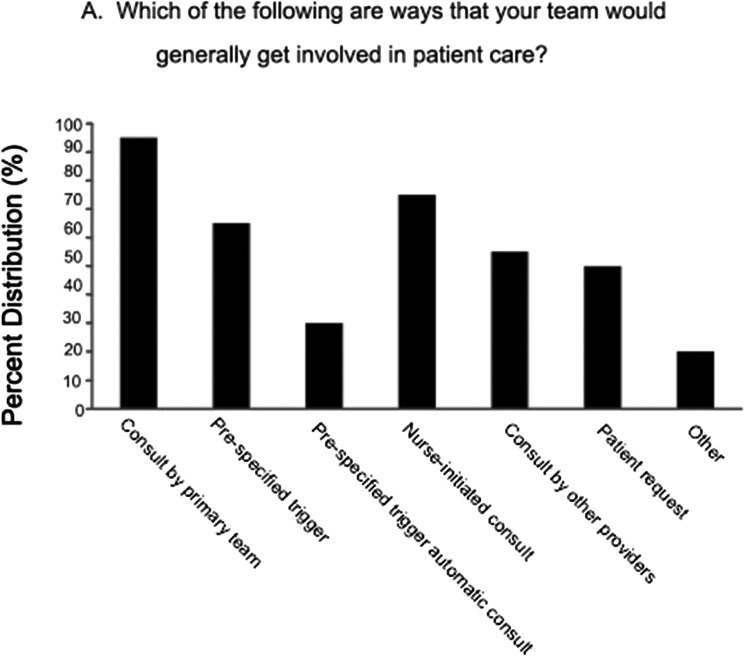
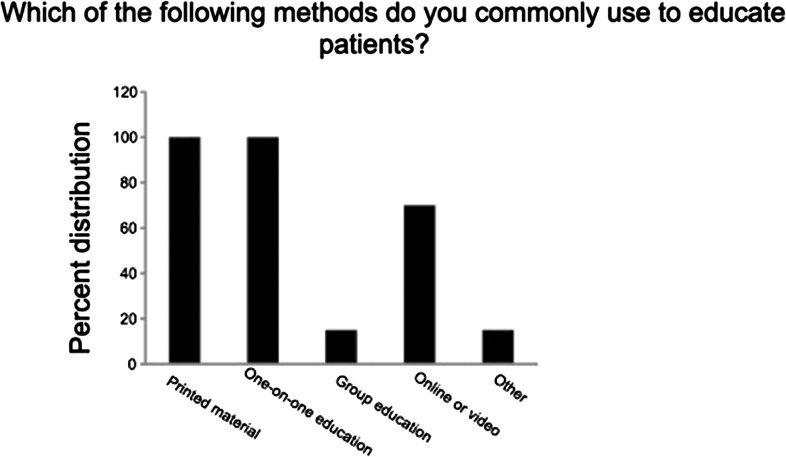
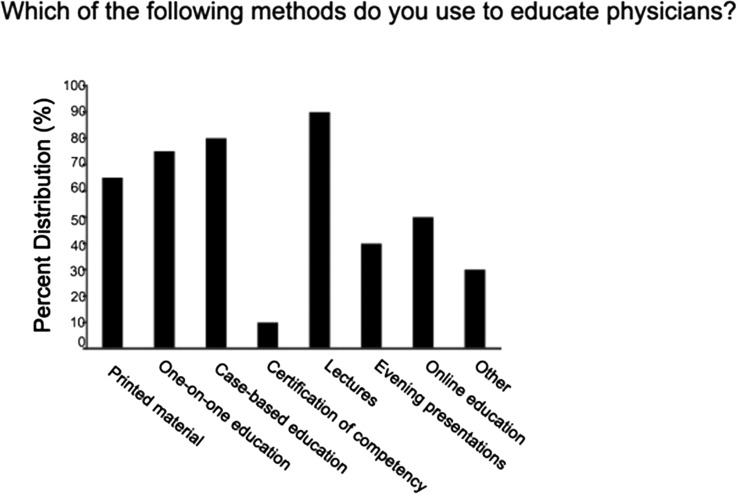
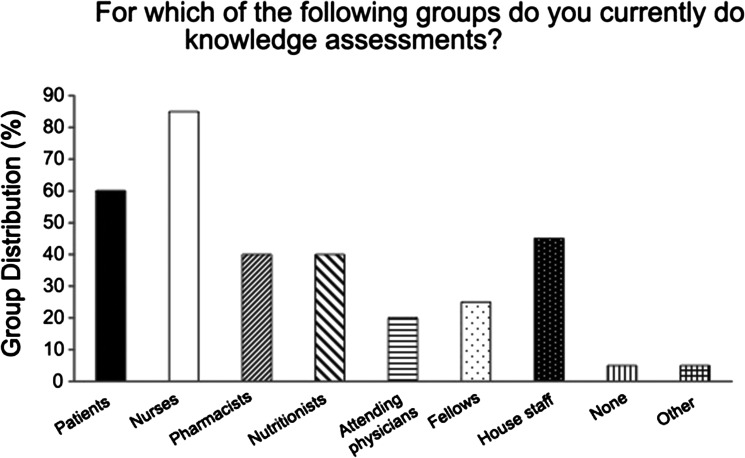
Objective. The Society for Hospital Medicine (SHM) conducted a survey of U.S. hospital systems to determine how nonphysician providers (NPPs) are utilized in interdisciplinary glucose management teams. Methods. An online survey grouped 50 questions into broad categories related to team functions. Queries addressed strategies that had proven successful, as well as challenges encountered. Fifty surveys were electronically distributed with an invitation to respond. A subset of seven respondents identified as having active glycemic committees that met at least every other month also participated in an in-depth telephone interview conducted by an SHM Glycemic Advisory Panel physician and NPP to obtain further details. The survey and interviews were conducted from May to July 2012. Results. Nineteen hospital/hospital system teams completed the survey (38% response rate). Most of the teams (52%) had existed for 1-5 years and served 90-100% of noncritical care, medical critical care, and surgical units. All of the glycemic control teams were supported by the use of protocols for insulin infusion, basal-bolus subcutaneous insulin orders, and hypoglycemia management. However, > 20% did not have protocols for discontinuation of oral hypoglycemic agents on admission or for transition from intravenous to subcutaneous insulin infusion. About 30% lacked protocols assessing A1C during the admission or providing guidance for insulin pump management. One-third reported that glycemic triggers led to preauthorized consultation or assumption of care for hyperglycemia. Institutional knowledge assessment programs were common for nurses (85%); intermediate for pharmacists, nutritionists, residents, and students (40-45%); and uncommon for fellows (25%) and attending physicians (20%). Many institutions were not monitoring appropriate use of insulin, oral agents, or insulin protocol utilization. Although the majority of teams had a process in place for post-discharge referrals and specific written instructions were provided, only one-fourth were supported with written protocols to standardize medication, education, equipment, and follow-up instructions. Conclusion. Inpatient glycemic control teams with NPPs often function in environments without a full set of measurement, education, standardization, transition, and order tools. Executive hospital leaders, community partners, and the glycemic control teams themselves need to address these deficiencies to optimize team effectiveness.
目的。医院医学协会(SHM)对美国医院系统进行了一项调查,以确定非医师提供者(NPP)在跨学科血糖管理团队中的使用情况。方法。一项在线调查将50个问题分为与团队功能相关的广泛类别。问题涉及已被证明成功的策略以及遇到的挑战。以电子方式分发了50份调查问卷并邀请作答。七名被确定为拥有至少每隔一个月开会一次的活跃血糖管理委员会的受访者组成的一个子集,还参与了由SHM血糖咨询小组的一名医生和NPP进行的深入电话访谈,以获取更多细节。调查和访谈于2012年5月至7月进行。结果。19个医院/医院系统团队完成了调查(回复率为38%)。大多数团队(52%)已经存在1至5年,服务于90%至100%的非重症监护、内科重症监护和外科病房。所有血糖控制团队都通过胰岛素输注方案、基础 - 餐时皮下胰岛素医嘱以及低血糖管理得到支持。然而,超过20%的团队没有关于入院时停用口服降糖药或从静脉胰岛素输注过渡到皮下胰岛素输注的方案。约30%的团队缺乏在入院期间评估糖化血红蛋白(A1C)或提供胰岛素泵管理指导的方案。三分之一的团队报告称血糖触发因素导致了针对高血糖的预先授权咨询或护理承担。机构知识评估项目对护士来说很常见(85%);对药剂师、营养师、住院医师和学生来说处于中等水平(40% - 45%);对研究员(25%)和主治医生(20%)来说则不常见。许多机构没有监测胰岛素、口服药物的合理使用或胰岛素方案的使用情况。虽然大多数团队有出院后转诊流程并提供了具体书面指示,但只有四分之一的团队有书面方案来规范药物、教育、设备和随访指示。结论。配备NPP的住院患者血糖控制团队通常在缺乏全套测量、教育、标准化转换和医嘱工具的环境中运作。医院行政领导、社区合作伙伴以及血糖控制团队自身需要解决这些不足,以优化团队效能。