Hartman Rebecca L, Brown Timothy L, Milavetz Gary, Spurgin Andrew, Gorelick David A, Gaffney Gary, Huestis Marilyn A
Chemistry and Drug Metabolism, Intramural Research Program, National Institute on Drug Abuse, NIH, Baltimore, MD, USA.
Program in Toxicology, University of Maryland, Baltimore, USA.
Drug Test Anal. 2016 Jul;8(7):690-701. doi: 10.1002/dta.1839. Epub 2015 Aug 10.
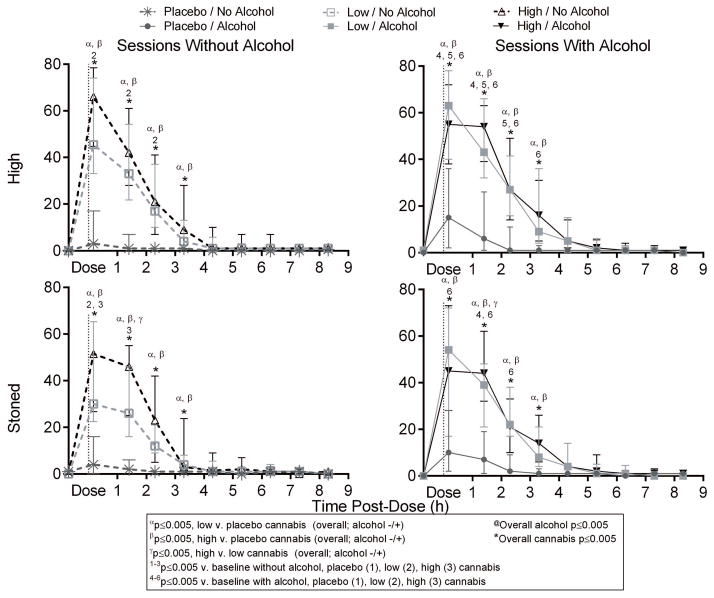
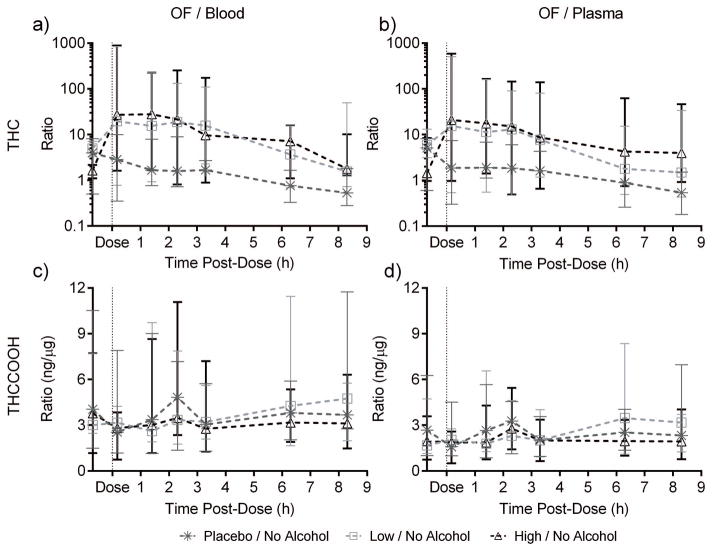
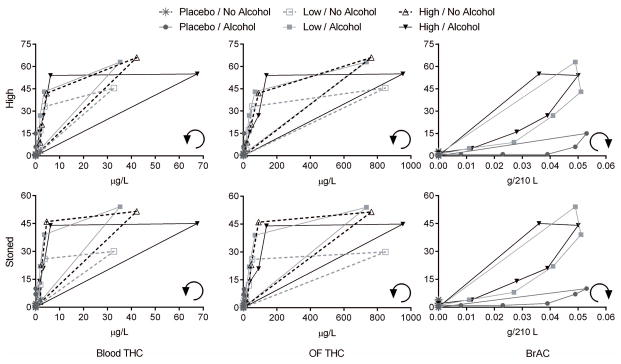
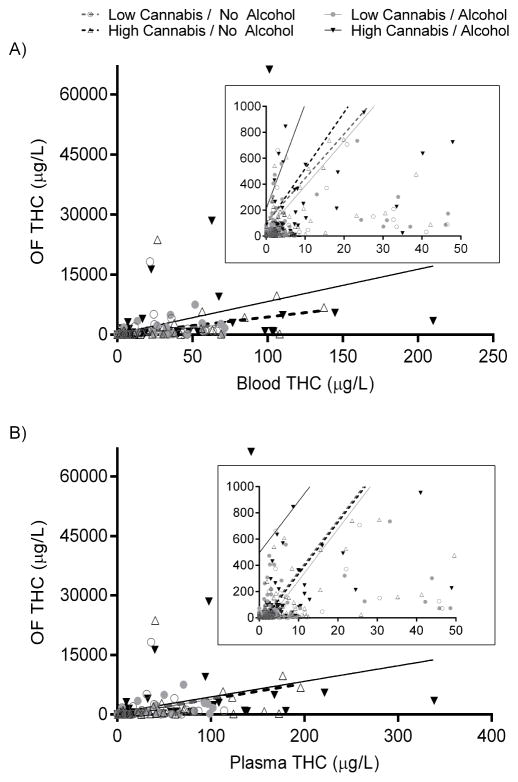
Vaporized cannabis and concurrent cannabis and alcohol intake are commonplace. We evaluated the subjective effects of cannabis, with and without alcohol, relative to blood and oral fluid (OF, advantageous for cannabis exposure screening) cannabinoid concentrations and OF/blood and OF/plasma vaporized-cannabinoid relationships. Healthy adult occasional-to-moderate cannabis smokers received a vaporized placebo or active cannabis (2.9% and 6.7% Δ(9) -tetrahydrocannabinol, THC) with or without oral low-dose alcohol (~0.065g/210L peak breath alcohol concentration [BrAC]) in a within-subjects design. Blood and OF were collected up to 8.3 h post-dose and subjective effects measured at matched time points with visual-analogue scales and 5-point Likert scales. Linear mixed models evaluated subjective effects by THC concentration, BrAC, and interactions. Effects by time point were evaluated by dose-wise analysis of variance (ANOVA). OF versus blood or plasma cannabinoid ratios and correlations were evaluated in paired-positive specimens. Nineteen participants (13 men) completed the study. Blood THC concentration or BrAC significantly associated with subjective effects including 'high', while OF contamination prevented significant OF concentration associations <1.4 h post-dose. Subjective effects persisted through 3.3-4.3 h, with alcohol potentiating the duration of the cannabis effects. Effect-versus-THC concentration and effect-versus-alcohol concentration hystereses were counterclockwise and clockwise, respectively. OF/blood and OF/plasma THC significantly correlated (all Spearman r≥0.71), but variability was high. Vaporized cannabis subjective effects were similar to those previously reported after smoking, with duration extended by concurrent alcohol. Cannabis intake was identified by OF testing, but OF concentration variability limited interpretation. Blood THC concentrations were more consistent across subjects and more accurate at predicting cannabis' subjective effects. Copyright © 2015 John Wiley & Sons, Ltd.
吸食大麻烟雾以及同时摄入大麻和酒精的情况很常见。我们评估了吸食大麻(无论是否同时饮酒)的主观效应,以及与之相关的血液和口腔液(OF,有利于大麻暴露筛查)中的大麻素浓度,还有口腔液与血液及口腔液与血浆中汽化大麻素的关系。健康的成年偶尔至中度吸食大麻者参与了一项自身对照设计的研究,他们接受了汽化安慰剂或活性大麻(Δ⁹ - 四氢大麻酚,THC含量分别为2.9%和6.7%),同时还接受了口服低剂量酒精(约0.065g/210L,呼气酒精浓度峰值[BrAC])或不接受酒精。给药后长达8.3小时采集血液和口腔液样本,并在匹配的时间点用视觉模拟量表和5点李克特量表测量主观效应。线性混合模型通过THC浓度、BrAC及其相互作用来评估主观效应。通过剂量方差分析(ANOVA)评估不同时间点的效应。在配对阳性样本中评估口腔液与血液或血浆大麻素的比率及相关性。19名参与者(13名男性)完成了该研究。血液THC浓度或BrAC与包括“兴奋”在内的主观效应显著相关,而给药后<1.4小时,口腔液污染导致口腔液浓度与主观效应无显著关联。主观效应持续3.3 - 4.3小时,酒精会延长大麻效应的持续时间。效应与THC浓度的滞后曲线呈逆时针方向,而效应与酒精浓度的滞后曲线呈顺时针方向。口腔液与血液及口腔液与血浆中的THC显著相关(所有Spearman相关系数r≥0.71),但变异性较高。吸食汽化大麻的主观效应与之前报道的吸烟后的效应相似,同时饮酒会延长效应持续时间。通过口腔液检测可确定大麻摄入情况,但口腔液浓度变异性限制了其解读。血液THC浓度在不同受试者之间更具一致性,并且在预测大麻的主观效应方面更准确。版权所有© 2015 John Wiley & Sons, Ltd.