Øvrehus Marius A, Zürbig Petra, Vikse Bjørn E, Hallan Stein I
Department of Nephrology, St Olav University Hospital, Trondheim, Norway ; Department of Cancer Research and Molecular Medicine, Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway.
Mosaiques Diagnostics GmbH, Hannover, Germany.
Clin Proteomics. 2015 Aug 7;12(1):21. doi: 10.1186/s12014-015-9092-7. eCollection 2015.
The contrast between a high prevalence of chronic kidney disease (CKD) and the low incidence of end-stage renal disease highlights the need for new biomarkers of progression beyond albuminuria testing. Urinary proteomics is a promising method, but more studies focusing on progression rate and patients with hypertensive nephropathy are needed.
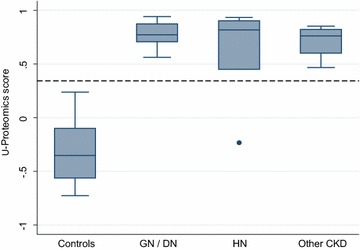
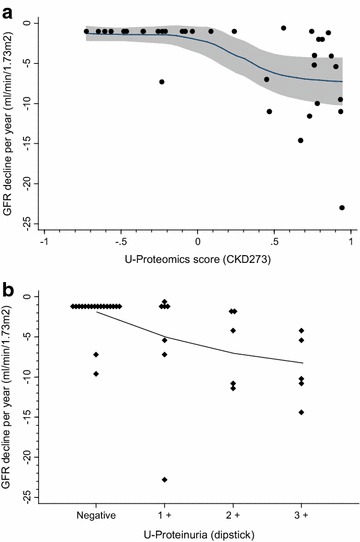
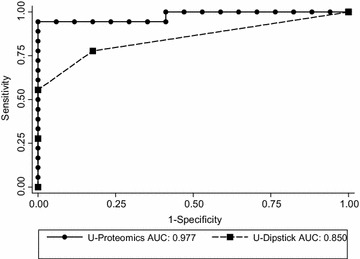
We analyzed urine samples with capillary electrophoresis coupled to a mass-spectrometer from 18 well characterized patients with CKD stage 4-5 (of whom six with hypertensive nephropathy) and 17 healthy controls. Classification scores based on a previously developed panel of 273 urinary peptides were calculated and compared to urine albumin dipstick results. Urinary proteomics classified CKD with a sensitivity of 0.95 and specificity of 1.00. Overall diagnostic accuracy (area under ROC curve) was 0.98, which was better than for albuminuria (0.85, p = 0.02). Results for hypertensive nephropathy were similar to other CKD diagnoses. Adding the proteomic score to an albuminuria model improved detection of rapid kidney function decline (>4 ml/min/1.73 m(2) per year) substantially: area under ROC curve increased from 0.762 to 0.909 (p = 0.042), and 38% of rapid progressors were correctly reclassified to a higher risk and 55% of slow progressors were correctly reclassified to a lower risk category. Reduced excretion of collagen types I-III, uromodulin, and other indicators of interstitial inflammation, fibrosis and tubular dysfunction were associated with CKD diagnosis and rapid progression. Patients with hypertensive nephropathy displayed the same findings as other types of CKD.
Urinary proteomic analyses had a high diagnostic accuracy for CKD, including hypertensive nephropathy, and strongly improved identification of patients with rapid kidney function decline beyond albuminuria testing.
慢性肾脏病(CKD)的高患病率与终末期肾病的低发病率之间的差异凸显了除蛋白尿检测之外,对新的疾病进展生物标志物的需求。尿液蛋白质组学是一种很有前景的方法,但需要更多关注进展率和高血压肾病患者的研究。
我们使用毛细管电泳与质谱联用技术分析了18例特征明确的4 - 5期CKD患者(其中6例患有高血压肾病)和17例健康对照者的尿液样本。计算基于先前开发的由273种尿肽组成的检测组的分类评分,并与尿白蛋白试纸条检测结果进行比较。尿液蛋白质组学对CKD的分类灵敏度为0.95,特异性为1.00。总体诊断准确性(ROC曲线下面积)为0.98,优于蛋白尿检测(0.85,p = 0.02)。高血压肾病的检测结果与其他CKD诊断相似。将蛋白质组学评分添加到蛋白尿模型中,可显著改善对肾功能快速下降(每年>4 ml/min/1.73 m²)的检测:ROC曲线下面积从0.762增加到0.909(p = 0.042),38%的快速进展者被正确重新分类为更高风险,55%的缓慢进展者被正确重新分类为更低风险类别。I - III型胶原蛋白、尿调节蛋白以及其他间质炎症、纤维化和肾小管功能障碍指标的排泄减少与CKD诊断和快速进展相关。高血压肾病患者与其他类型的CKD表现相同。
尿液蛋白质组学分析对CKD(包括高血压肾病)具有较高的诊断准确性,并且在蛋白尿检测之外,能显著改善对肾功能快速下降患者的识别。