Smith Tyler, Samandari Taraz, Abimbola Taiwo, Marston Barbara, Sangrujee Nalinee
*Division of Global HIV/AIDS, US Centers for Disease Control and Prevention (CDC); and †Division of Tuberculosis Elimination, US Centers for Disease Control and Prevention (CDC).
J Acquir Immune Defic Syndr. 2015 Nov 1;70(3):e84-93. doi: 10.1097/QAI.0000000000000783.
In Botswana, a 36-month course of isoniazid treatment of latent tuberculosis (TB) infection [isoniazid preventive therapy (IPT)] was superior to 6-month IPT in reducing TB and death in persons living with HIV (PLHIV), having positive tuberculin skin tests (TSTs) but not in those with negative TST. We examined the cost-effectiveness of IPT in Botswana, where antiretroviral therapy (ART) is widely available.
Using a decision-analytic model, we determined the incremental cost-effectiveness of strategies for reducing TB and death in 10,000 PLHIV over 36 months.
IPT for 6 months and provision of ART if CD4 lymphocyte count <250 cells per microliter (2011 Botswana policy) was compared with 6 alternative strategies that varied the use of IPT, TST, and ART for CD4 count thresholds, including CD4 <350 and <500 cells per microliter.
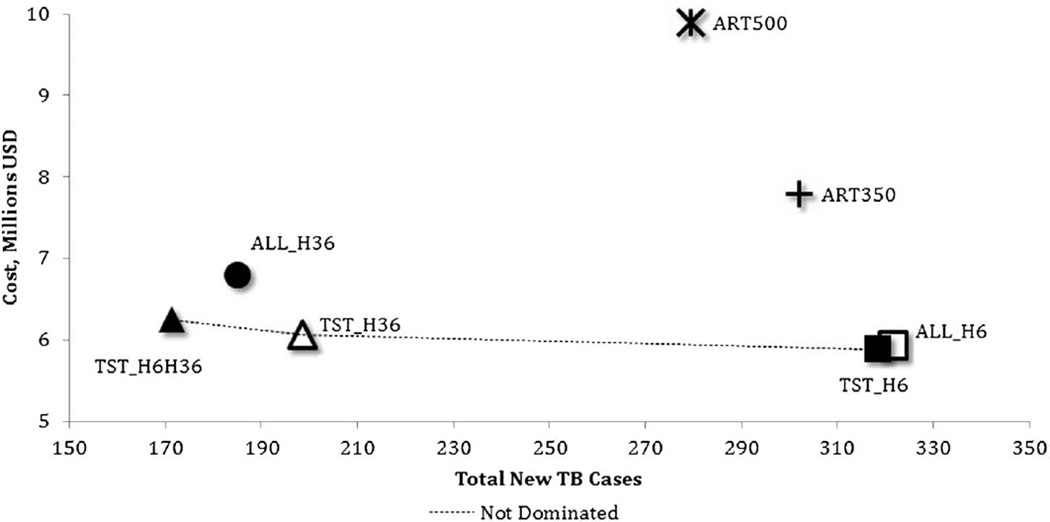
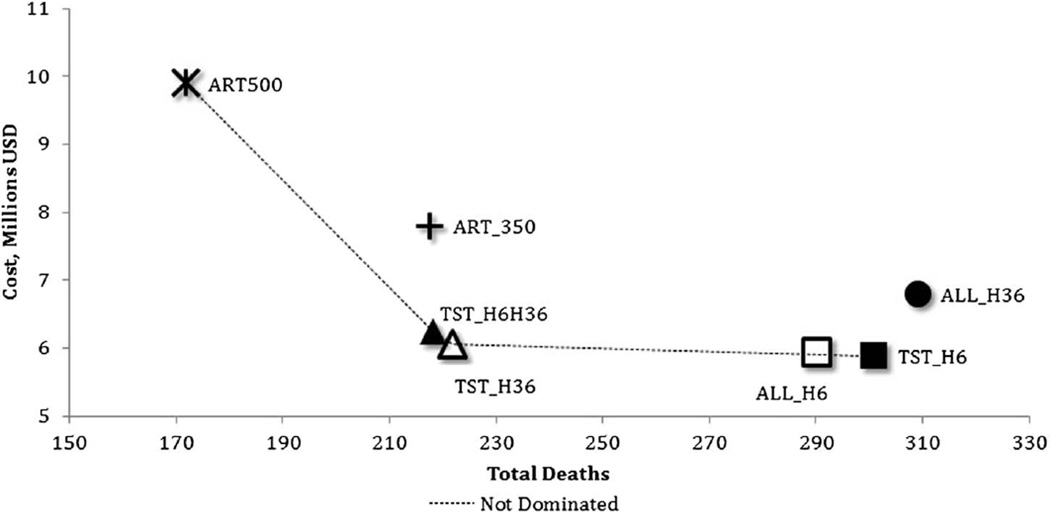
Botswana policy, 2011 was dominated by most other strategies. IPT of 36 months for TST-positive PLHIV with ART for CD4 <250 cells per microliter resulted in 120 fewer TB cases for an additional cost of $1612 per case averted and resulted in 80 fewer deaths for an additional $2418 per death averted compared with provision of 6-month IPT to TST-positive PLHIV who received ART for CD4 <250 cells per microliter, the next most effective strategy. Alternative strategies offered lower incremental effectiveness at higher cost. These findings remained consistent in sensitivity analyses.
A strategy of treating PLHIV who have positive TST with 36-month IPT is more cost effective for reducing both TB and death compared with providing IPT without a TST, providing only 6-month IPT, or expanding ART eligibility without IPT.
在博茨瓦纳,对潜伏性结核感染进行36个月的异烟肼治疗[异烟肼预防性治疗(IPT)]在降低结核病发病率及死亡率方面优于6个月的IPT,该治疗针对结核菌素皮肤试验(TST)呈阳性的艾滋病毒感染者(PLHIV),但对TST呈阴性者效果不佳。我们研究了在博茨瓦纳广泛提供抗逆转录病毒治疗(ART)的情况下IPT的成本效益。
使用决策分析模型,我们确定了在36个月内降低10,000名PLHIV结核病发病率及死亡率的策略的增量成本效益。
将6个月的IPT以及CD4淋巴细胞计数<250个/微升时提供ART(2011年博茨瓦纳政策)与6种替代策略进行比较,这些替代策略在IPT、TST的使用以及针对不同CD4计数阈值(包括CD4<350和<500个/微升)的ART使用方面存在差异。
2011年的博茨瓦纳政策在大多数其他策略中处于劣势。与为CD4<250个/微升且TST呈阳性的PLHIV提供6个月IPT(次最有效策略)相比,为CD4<250个/微升且TST呈阳性的PLHIV提供36个月IPT并联合ART,每避免一例结核病病例需额外花费1612美元,结核病病例减少120例;每避免一例死亡需额外花费2418美元,死亡病例减少80例。替代策略在成本更高的情况下提供的增量效果更低。这些发现在敏感性分析中保持一致。
与不进行TST就提供IPT、仅提供6个月IPT或在不进行IPT的情况下扩大ART资格相比,对TST呈阳性的PLHIV采用36个月IPT治疗的策略在降低结核病发病率及死亡率方面更具成本效益。