Health Economics Unit, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, Anzio Road, Cape Town, South Africa.
Department of Global Health and Development, Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, UK.
Pharmacoeconomics. 2020 Aug;38(8):819-837. doi: 10.1007/s40273-020-00910-w.
There is a need for easily accessible tuberculosis unit cost data, as well as an understanding of the variability of methods used and reporting standards of that data.
The aim of this systematic review was to descriptively review papers reporting tuberculosis unit costs from a healthcare provider perspective looking at methodological variation; to assess quality using a study quality rating system and machine learning to investigate the indicators of reporting quality; and to identify the data gaps to inform standardised tuberculosis unit cost collection and consistent principles for reporting going forward.
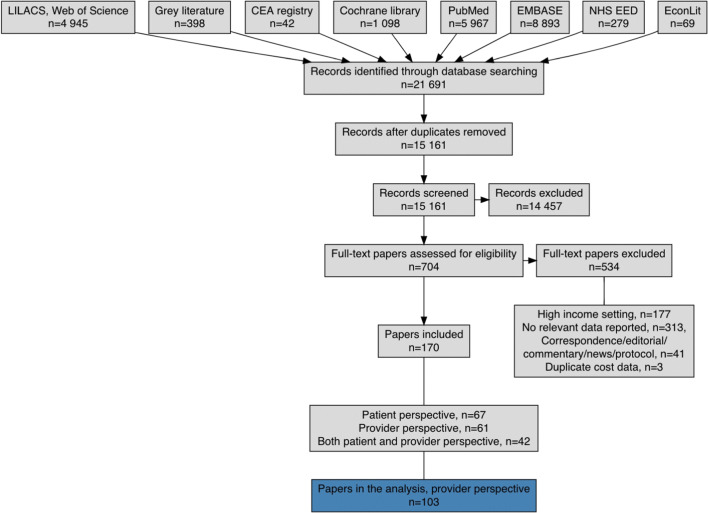
We searched grey and published literature in five sources and eight databases, respectively, using search terms linked to cost, tuberculosis and tuberculosis health services including tuberculosis treatment and prevention. For inclusion, the papers needed to contain empirical unit cost estimates for tuberculosis interventions from low- and middle-income countries, with reference years between 1990 and 2018. A total of 21,691 papers were found and screened in a phased manner. Data were extracted from the eligible papers into a detailed Microsoft Excel tool, extensively cleaned and analysed with R software (R Project, Vienna, Austria) using the user interface of RStudio. A study quality rating was applied to the reviewed papers based on the inclusion or omission of a selection of variables and their relative importance. Following this, machine learning using a recursive partitioning method was utilised to construct a classification tree to assess the reporting quality.
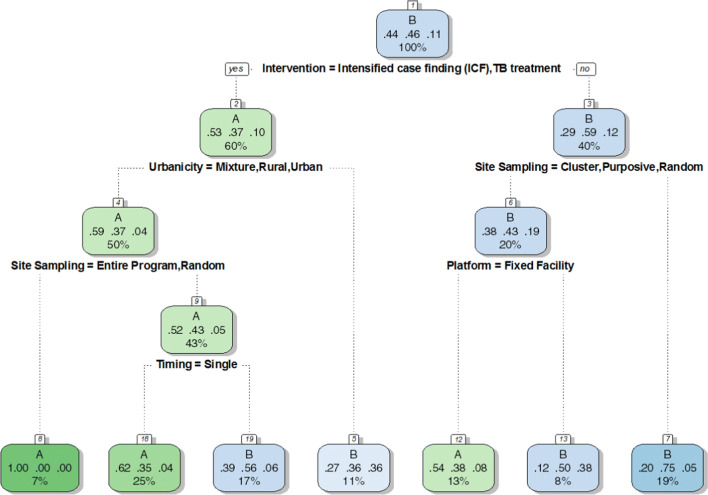
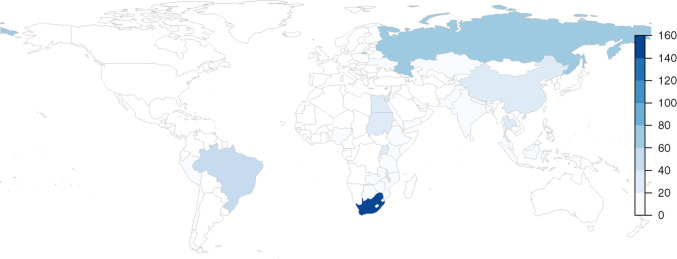
This systematic review included 103 provider perspective papers with 627 unit costs (costs not presented here) for tuberculosis interventions among a total of 140 variables. The interventions covered were active, passive and intensified case finding; tuberculosis treatment; above-service costs; and tuberculosis prevention. Passive case finding is the detection of tuberculosis cases where individuals self-identify at health facilities; active case finding is detection of cases of those not in health facilities, such as through outreach; and intensified case finding is detection of cases in high-risk populations. There was heterogeneity in some of the reported methods used such cost allocation, amortisation and the use of top-down, bottom-up or mixed approaches to the costing. Uncertainty checking through sensitivity analysis was only reported on by half of the papers (54%), while purposive and convenience sampling was reported by 72% of papers. Machine learning indicated that reporting on 'Intervention' (in particular), 'Urbanicity' and 'Site Sampling', were the most likely indicators of quality of reporting. The largest data gap identified was for tuberculosis vaccination cost data, the Bacillus Calmette-Guérin (BCG) vaccine in particular. There is a gap in available unit costs for 12 of 30 high tuberculosis burden countries, as well as for the interventions of above-service costs, tuberculosis prevention, and active and intensified case finding.
Variability in the methods and reporting used makes comparison difficult and makes it hard for decision makers to know which unit costs they can trust. The study quality rating system used in this review as well as the classification tree enable focus on specific reporting aspects that should improve variability and increase confidence in unit costs. Researchers should endeavour to be explicit and transparent in how they cost interventions following the principles as laid out in the Global Health Cost Consortium's Reference Case for Estimating the Costs of Global Health Services and Interventions, which in turn will lead to repeatability, comparability and enhanced learning from others.
需要方便获取结核病单位成本数据,并且需要了解所使用方法的可变性和报告这些数据的标准。
本系统评价旨在从医疗保健提供者的角度描述性地审查报告结核病单位成本的论文,着眼于方法学的变化;使用研究质量评分系统进行评估,并使用机器学习来调查报告质量的指标;确定数据空白,以便为今后的标准化结核病单位成本收集和一致的报告原则提供信息。
我们在五个来源中分别使用与成本、结核病和结核病卫生服务(包括结核病治疗和预防)相关的搜索词,在八个数据库中搜索灰色和已发表文献。为了纳入研究,论文需要包含来自中低收入国家的结核病干预措施的经验性单位成本估算,并参考 1990 年至 2018 年的年份。共发现并分阶段筛选了 21691 篇论文。从合格的论文中提取数据到一个详细的 Microsoft Excel 工具中,使用 R 软件(奥地利维也纳的 R 项目)使用 RStudio 的用户界面进行广泛的清理和分析。根据所包含或遗漏的变量及其相对重要性,对所审查的论文进行研究质量评分。随后,使用递归分区方法的机器学习用于构建分类树来评估报告质量。
本系统评价共纳入 103 篇从提供者角度出发的论文,其中有 627 项结核病干预措施的单位成本(此处未提供成本),共有 140 个变量。所涵盖的干预措施包括主动、被动和强化病例发现;结核病治疗;服务外成本;以及结核病预防。被动病例发现是指在医疗机构中自我识别的结核病病例的检测;主动病例发现是指在医疗机构外发现的病例的检测,例如通过外展;强化病例发现是指在高危人群中发现病例。所报告的一些方法的使用存在异质性,例如成本分配、摊销以及自上而下、自下而上或混合的成本核算方法。只有一半(54%)的论文报告了通过敏感性分析进行不确定性检查,而 72%的论文报告了有目的和便利抽样。机器学习表明,“干预”(特别是)、“城市”和“采样地点”的报告是报告质量的最可能指标。确定的最大数据空白是卡介苗(BCG)疫苗等结核病疫苗的接种成本数据。在 30 个结核病负担较高的国家中,有 12 个国家缺乏可用的单位成本数据,同时缺乏服务外成本、结核病预防以及主动和强化病例发现方面的单位成本数据。
所使用方法和报告的可变性使得比较变得困难,决策者也难以知道他们可以信任哪些单位成本。本研究中使用的研究质量评分系统以及分类树使人们能够专注于特定的报告方面,从而提高可变性并增加对单位成本的信心。研究人员应努力按照全球卫生成本联合会(Global Health Cost Consortium)的“估算全球卫生服务和干预措施成本参考案例”中规定的原则来明确和透明地对干预措施进行成本核算,这反过来又将提高可重复性、可比性并增强从他人处学习的能力。