Cairns Matthew E, Walker Patrick G T, Okell Lucy C, Griffin Jamie T, Garske Tini, Asante Kwaku Poku, Owusu-Agyei Seth, Diallo Diadier, Dicko Alassane, Cisse Badara, Greenwood Brian M, Chandramohan Daniel, Ghani Azra C, Milligan Paul J
MRC Tropical Epidemiology Group, LSHTM, London, UK.
MRC Centre for Outbreak Analysis and Modelling, Imperial College London, London, UK.
Malar J. 2015 Aug 19;14:321. doi: 10.1186/s12936-015-0839-4.
Long-acting artemisinin-based combination therapy (LACT) offers the potential to prevent recurrent malaria attacks in highly exposed children. However, it is not clear where this advantage will be most important, and deployment of these drugs is not rationalized on this basis.
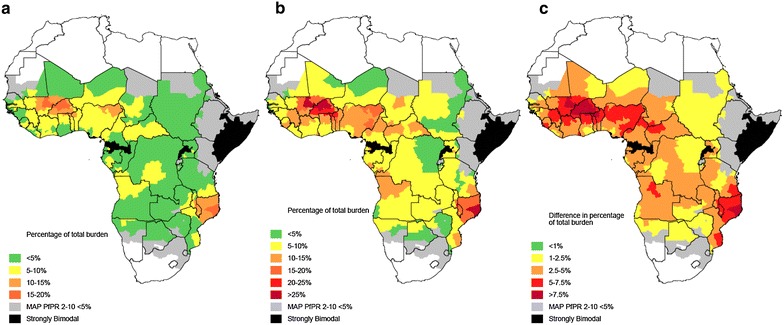
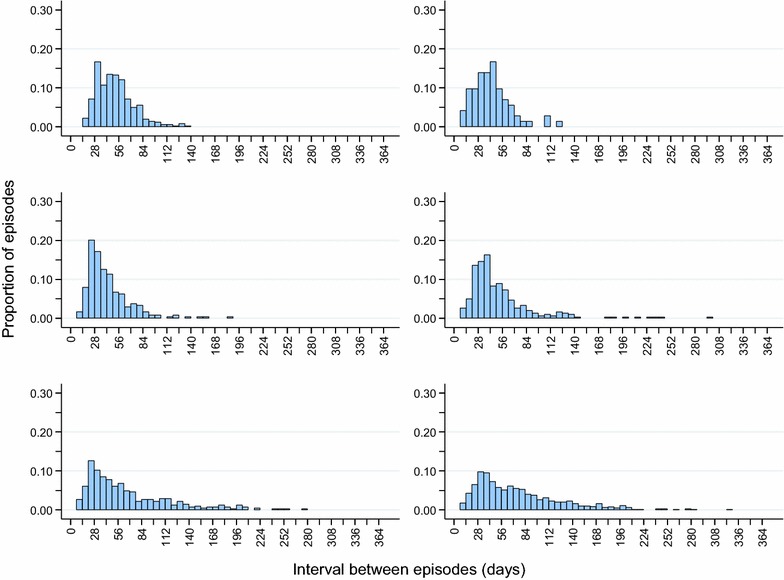
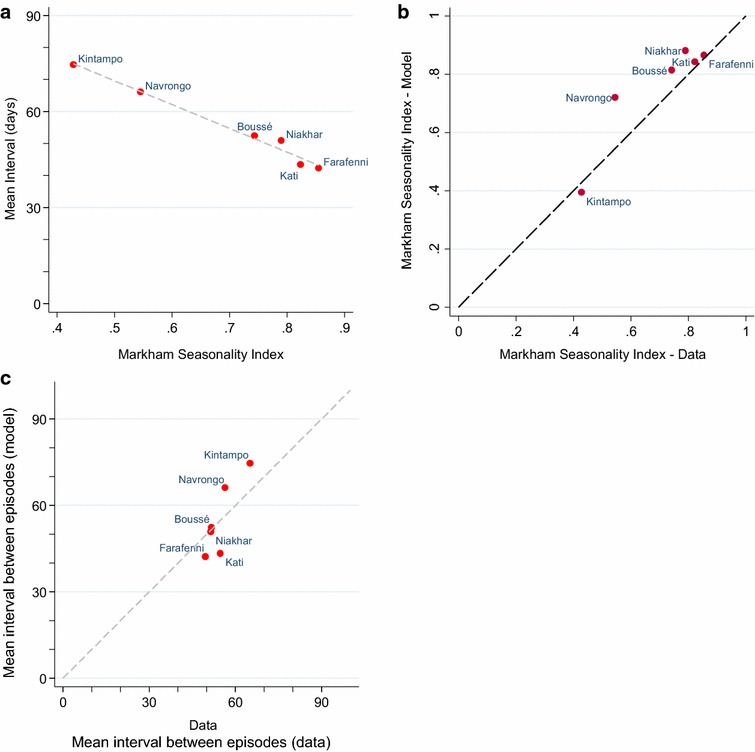
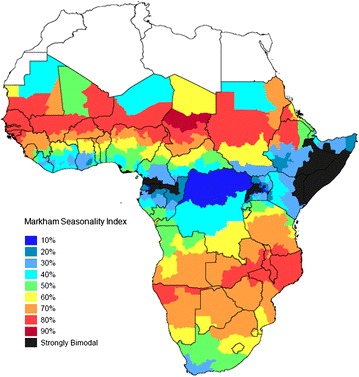
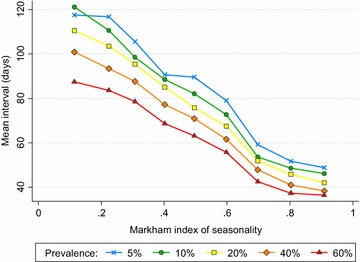
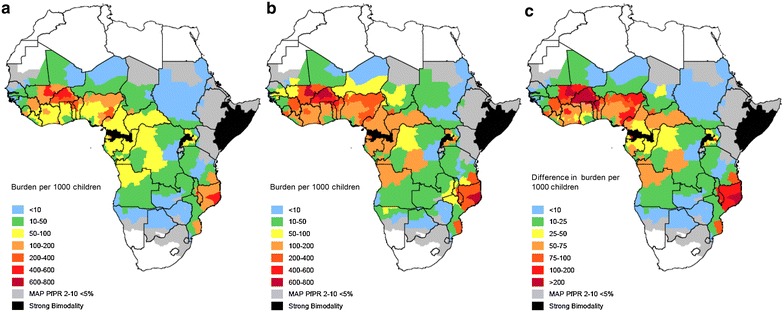
To understand where post-treatment prophylaxis would be most beneficial, the relationship between seasonality, transmission intensity and the interval between malaria episodes was explored using data from six cohort studies in West Africa and an individual-based malaria transmission model. The total number of recurrent malaria cases per 1000 child-years at risk, and the fraction of the total annual burden that this represents were estimated for sub-Saharan Africa.
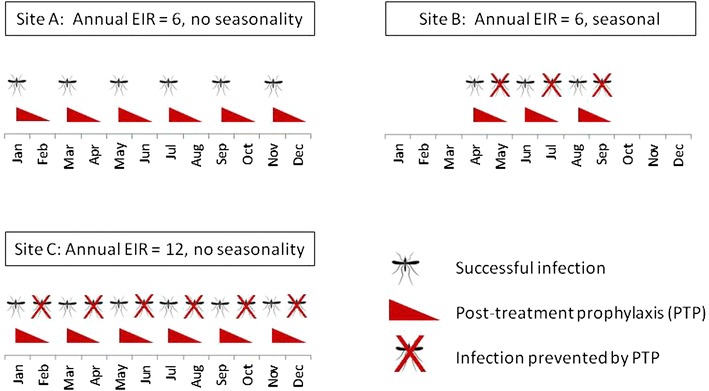
In settings where prevalence is less than 10 %, repeat malaria episodes constitute a small fraction of the total burden, and few repeat episodes occur within the window of protection provided by currently available drugs. However, in higher transmission settings, and particularly in high transmission settings with highly seasonal transmission, repeat malaria becomes increasingly important, with up to 20 % of the total clinical burden in children estimated to be due to repeat episodes within 4 weeks of a prior attack.
At a given level of transmission intensity and annual incidence, the concentration of repeat malaria episodes in time, and consequently the protection from LACT is highest in the most seasonal areas. As a result, the degree of seasonality, in addition to the overall intensity of transmission, should be considered by policy makers when deciding between ACT that differ in their duration of post-treatment prophylaxis.
长效青蒿素联合疗法(LACT)有可能预防高度暴露儿童的疟疾复发。然而,尚不清楚这种优势在何处最为重要,且这些药物的部署并未基于此进行合理规划。
为了解治疗后预防措施在何处最为有益,利用来自西非六项队列研究的数据和基于个体的疟疾传播模型,探讨了季节性、传播强度与疟疾发作间隔之间的关系。估计了撒哈拉以南非洲每1000儿童年风险中复发性疟疾病例的总数,以及这在年度总负担中所占的比例。
在患病率低于10%的地区,复发性疟疾发作占总负担的比例较小,且在现有药物提供的保护期内很少发生复发性发作。然而,在传播率较高的地区,尤其是在传播高度季节性的高传播地区,复发性疟疾变得越来越重要,估计高达20%的儿童临床总负担是由于在先前发作后4周内的复发性发作所致。
在给定的传播强度和年发病率水平下,复发性疟疾发作在时间上的集中程度,以及因此从LACT获得的保护在季节性最强的地区最高。因此,政策制定者在决定治疗后预防期不同的青蒿素联合疗法时,除了考虑总体传播强度外,还应考虑季节性程度。