Gilardoni Elisa, Bernasconi Davide Paolo, Poli Silvia, Garancini Mattia, Luperto Margherita, Zucchini Nicola, Bovo Giorgio, Totis Mauro, Bugatti Alvaro, Gianotti Luca
Department of Surgery and Translational Medicine, Milano-Bicocca University, San Gerardo Hospital, Monza, Italy.
Department of Health Science, Centre of Biostatistics for Clinical Epidemiology, Milano-Bicocca University, Monza, Italy.
World J Surg Oncol. 2015 Aug 28;13:260. doi: 10.1186/s12957-015-0674-7.
Although several meta-analyses showed the positive effects of follow-up on the prognosis of colon cancer (CC), international guidelines are not in accordance on appropriate tests and their time frequency to optimize surveillance. Furthermore, stratified strategies based upon risk grading have not been implemented. This approach may be useful to rationalize resources.
From 2006, all patients operated for an early stage CC (I, IIA, IIB) according to the 7th edition of the AJCC-2010 classification entered in a prospective surveillance program in accordance to our local guidelines. Patients who underwent surgical resection after 2009 have been excluded to guarantee at least a 5-year follow-up. Classic histopathologic prognostic factors such as grade, T and N status, lymphatic and vascular invasion were assessed. Moreover, tumor budding and tumor-to-stroma proportion were evaluated.
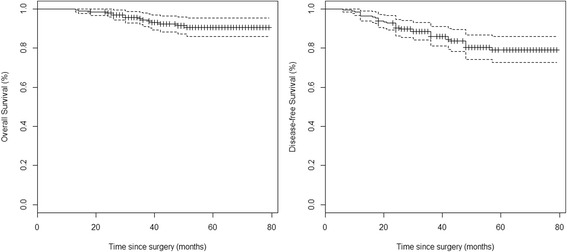
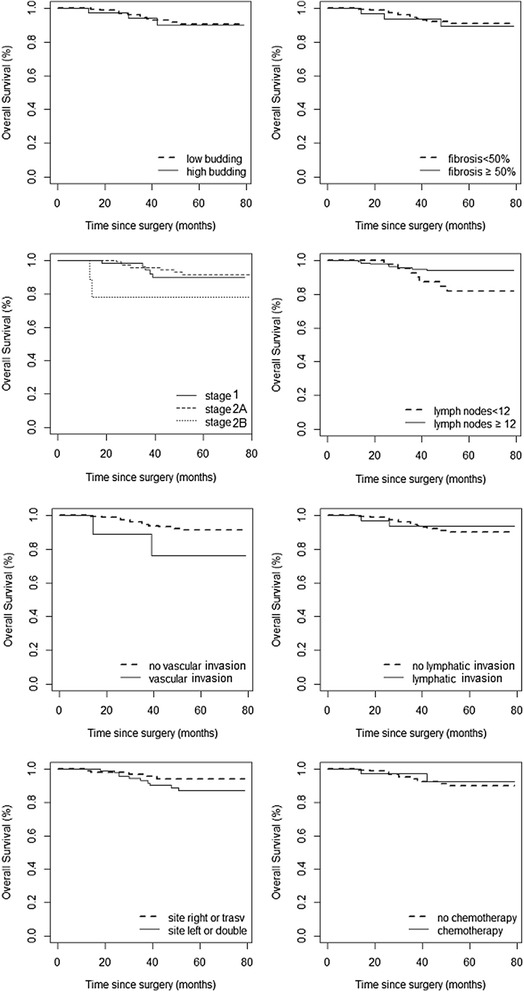
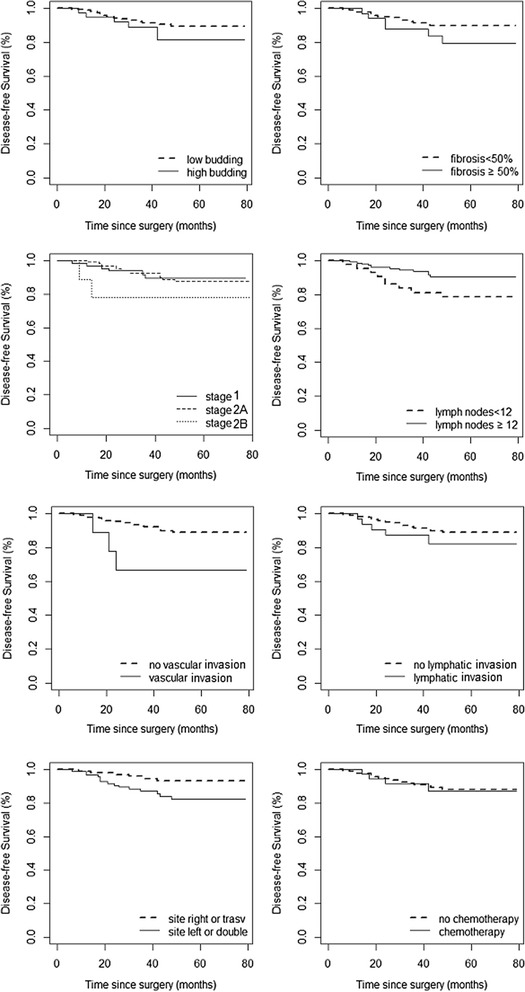
We had complete records of 196 patients. Distribution was as follows: 65 (33.2%) in stage I, 122 (62.2%) in stage IIA, and 9 (4.6%) in stage IIB. Eleven patients (5.6%) had a disease recurrence (local or distant). The median recurrence time was 20 months (range 6-48). Nine patients (82%) had recurrence with 24 months, and 91% were asymptomatic and detected by ultrasound or CT scan. According to the log-rank test, the risk factors with significant effect on the disease-free survival (DFS) were the number of lymph nodes <12 (p = 0.027) and the vascular invasion (p = 0.021), while for the overall (OS), only the vascular invasion was significant (p = 0.043). By the univariate and multivariate analyses, DSF was significantly lower in patients with less than 12 nodes removed, with vascular invasion, and with left of double cancer. OS was negatively affected only by vascular invasion despite the hazard ratios were similar to DSF. Stage IIB was associated with a threefold-increased risk of reduced OS and DSF.
Stages I and IIA appear to behave similarly and should be considered as true early stages. The detection of fibrosis and budding do not seem to add valuable information for prognosis. In early CC stages, the surveillance program should be maximized within the first two years.
尽管多项荟萃分析显示随访对结肠癌(CC)预后有积极影响,但国际指南在优化监测的适当检查及其时间频率方面并未达成一致。此外,基于风险分级的分层策略尚未实施。这种方法可能有助于合理配置资源。
自2006年起,所有根据2010年美国癌症联合委员会(AJCC)第7版分类接受早期CC(I、IIA、IIB期)手术的患者均按照我们当地的指南进入前瞻性监测计划。2009年后接受手术切除的患者被排除在外,以确保至少有5年的随访。评估了经典的组织病理学预后因素,如分级、T和N分期、淋巴和血管侵犯。此外,还评估了肿瘤芽生和肿瘤与基质比例。
我们有196例患者的完整记录。分布如下:I期65例(33.2%),IIA期122例(62.2%),IIB期9例(4.6%)。11例患者(5.6%)出现疾病复发(局部或远处)。中位复发时间为20个月(范围6 - 48个月)。9例患者(82%)在24个月内复发,91%无症状,通过超声或CT扫描检测到。根据对数秩检验,对无病生存期(DFS)有显著影响的危险因素是淋巴结数量<12个(p = 0.027)和血管侵犯(p = 0.021),而对于总生存期(OS),只有血管侵犯具有显著性(p = 0.043)。通过单因素和多因素分析,切除淋巴结少于12个、有血管侵犯以及双癌左侧的患者DFS显著较低。尽管危险比与DFS相似,但OS仅受血管侵犯的负面影响。IIB期与OS和DFS降低的风险增加三倍相关。
I期和IIA期表现似乎相似,应被视为真正的早期阶段。纤维化和芽生的检测似乎并未为预后增加有价值的信息。在早期CC阶段,监测计划应在前两年内最大化。