Lehnen Nadine, Heuser Fabian, Sağlam Murat, Schulz Christian M, Wagner Klaus J, Taki Masakatsu, Kochs Eberhard F, Jahn Klaus, Brandt Thomas, Glasauer Stefan, Schneider Erich
Centre for Sensorimotor Research, Munich University Hospital, Munich, Germany; German Centre for Vertigo and Balance Disorders, Munich University Hospital, Munich, Germany; Department of Neurology, Munich University Hospital, Munich, Germany.
Department of Anaesthesiology, Klinikum rechts der Isar, Technische Universität München, Munich, Germany.
PLoS One. 2015 Aug 27;10(8):e0135263. doi: 10.1371/journal.pone.0135263. eCollection 2015.
Opioids are indispensable for pain treatment but may cause serious nausea and vomiting. The mechanism leading to these complications is not clear. We investigated whether an opioid effect on the vestibular system resulting in corrupt head motion sensation is causative and, consequently, whether head-rest prevents nausea.
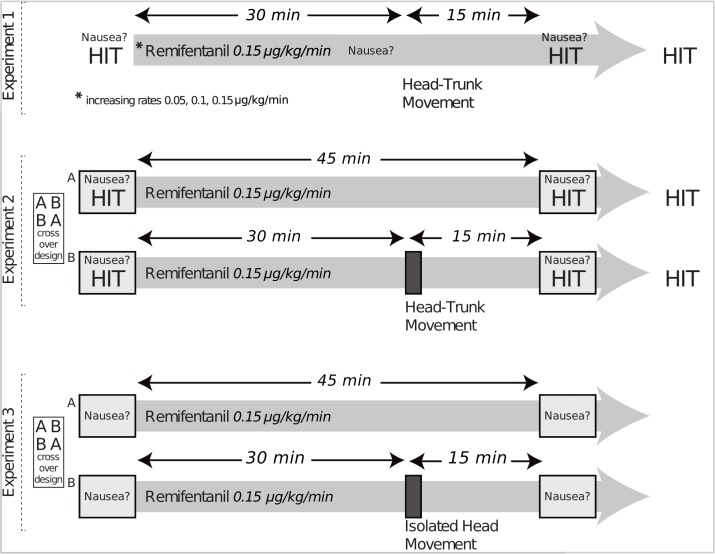
Thirty-six healthy men (26.6 ± 4.3 years) received an opioid remifentanil infusion (45 min, 0.15 μg/kg/min). Outcome measures were the vestibulo-ocular reflex (VOR) gain determined by video-head-impulse-testing, and nausea. The first experiment (n = 10) assessed outcome measures at rest and after a series of five 1-Hz forward and backward head-trunk movements during one-time remifentanil administration. The second experiment (n = 10) determined outcome measures on two days in a controlled crossover design: (1) without movement and (2) with a series of five 1-Hz forward and backward head-trunk bends 30 min after remifentanil start. Nausea was psychophysically quantified (scale from 0 to 10). The third controlled crossover experiment (n = 16) assessed nausea (1) without movement and (2) with head movement; isolated head movements consisting of the three axes of rotation (pitch, roll, yaw) were imposed 20 times at a frequency of 1 Hz in a random, unpredictable order of each of the three axes. All movements were applied manually, passively with amplitudes of about ± 45 degrees.
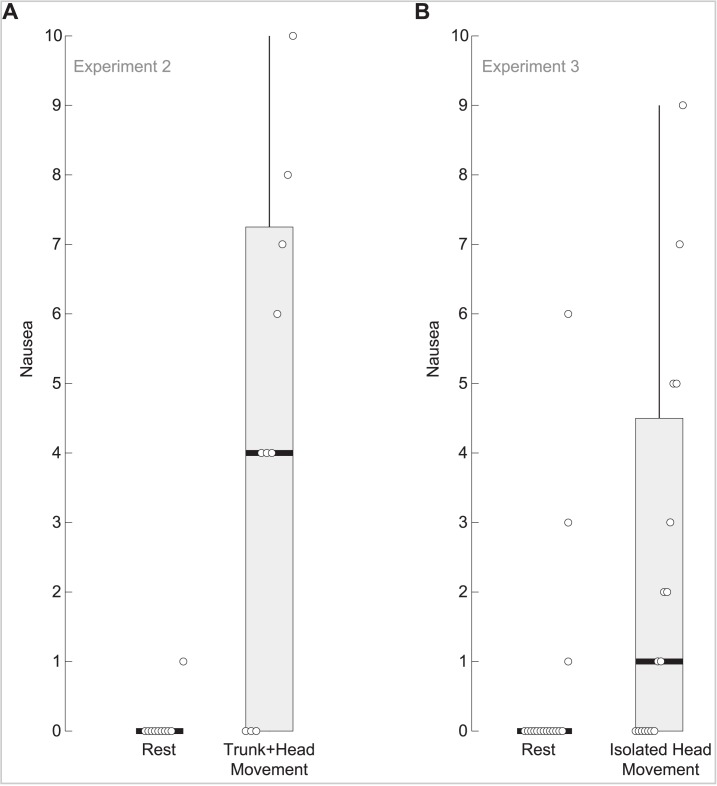
The VOR gain decreased during remifentanil administration (p<0.001), averaging 0.92 ± 0.05 (mean ± standard deviation) before, 0.60 ± 0.12 with, and 0.91 ± 0.05 after infusion. The average half-life of VOR recovery was 5.3 ± 2.4 min. 32/36 subjects had no nausea at rest (nausea scale 0.00/0.00 median/interquartile range). Head-trunk and isolated head movement triggered nausea in 64% (p<0.01) with no difference between head-trunk and isolated head movements (nausea scale 4.00/7.25 and 1.00/4.5, respectively).
Remifentanil reversibly decreases VOR gain at a half-life reflecting the drug's pharmacokinetics. We suggest that the decrease in VOR gain leads to a perceptual mismatch of multisensory input with the applied head movement, which results in nausea, and that, consequently, vigorous head movements should be avoided to prevent opioid-induced nausea.
阿片类药物是疼痛治疗中不可或缺的,但可能会引起严重的恶心和呕吐。导致这些并发症的机制尚不清楚。我们研究了阿片类药物对前庭系统产生异常头部运动感觉的影响是否是其病因,以及因此头部固定是否能预防恶心。
36名健康男性(26.6±4.3岁)接受瑞芬太尼静脉输注(45分钟,0.15μg/kg/分钟)。观察指标为通过视频头脉冲测试确定的前庭眼反射(VOR)增益和恶心情况。第一个实验(n = 10)在单次给予瑞芬太尼期间,评估静息状态下以及一系列五次1赫兹前后头部 - 躯干运动后的观察指标。第二个实验(n = 10)采用对照交叉设计在两天内确定观察指标:(1)无运动时;(2)瑞芬太尼开始输注30分钟后进行一系列五次1赫兹前后头部 - 躯干弯曲时。恶心情况通过心理物理学方法进行量化(0至10分)。第三个对照交叉实验(n = 16)评估(1)无运动时和(2)有头部运动时的恶心情况;由三个旋转轴(俯仰、横滚、偏航)组成的孤立头部运动以1赫兹的频率随机、不可预测地各施加20次。所有运动均由人工被动施加,幅度约为±45度。
在输注瑞芬太尼期间VOR增益降低(p<0.001),输注前平均为0.92±0.05(均值±标准差),输注时为0.60±0.12,输注后为0.91±'0.05。VOR恢复的平均半衰期为5.3±2.4分钟。36名受试者中有32名在静息时无恶心(恶心评分为0.00/0.00中位数/四分位间距)。头部 - 躯干运动和孤立头部运动在64%的受试者中引发恶心(p<0.01),头部 - 躯干运动和孤立头部运动之间无差异(恶心评分分别为4.00/7.25和1.00/4.5)。
瑞芬太尼以反映药物药代动力学的半衰期可逆地降低VOR增益。我们认为VOR增益的降低导致多感觉输入与所施加的头部运动之间的感知不匹配,从而导致恶心,因此应避免剧烈头部运动以预防阿片类药物引起的恶心。