Du Shunda, Ni Jianjiao, Weng Linqian, Ma Fei, Li Shaohua, Wang Wenze, Sang Xinting, Lu Xin, Zhong Shouxian, Mao Yilei
From the Department of Liver Surgery (SD, JN, LW, XS, XL, SZ, YM); Department of Medical Oncology, Cancer Hospital and Institute, Chinese Academy of Medical Sciences and PUMC, Beijing (FM); Department of Hepatobiliary Surgery, Sun Yat-sen University Cancer Center, Guangzhou (SL); and Department of Pathology, Peking Union Medical College (PUMC) Hospital, Chinese Academy of Medical Sciences and PUMC, Beijing, China (WW).
Medicine (Baltimore). 2015 Aug;94(34):e1429. doi: 10.1097/MD.0000000000001429.
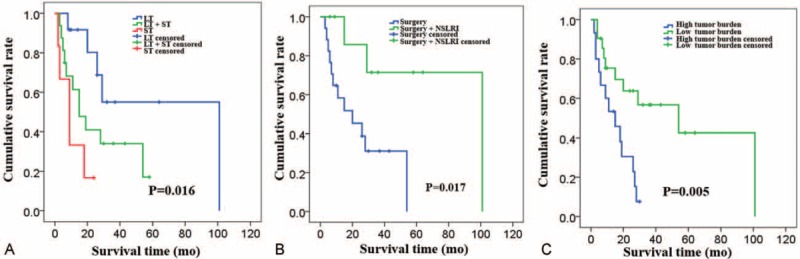
Grade 3 (G3) gastroenteropancreatic (GEP) neuroendocrine tumors (NETs) are rare, and there is no report specifically dealing with patients of liver metastases from G3 GEP NETs.From January 2004 to January 2014, 36 conservative patients with G3 GEP NET liver metastases were retrospectively identified from 3 hepatobiliary centers in China. The clinical features and treatment outcomes were analyzed.Aggressive locoregional treatments (LT, including cytoreductive surgery, radiofrequency ablation, and liver-directed intra-arterial intervention) and systemic therapy (ST) were introduced separately or combined, with 26 (72%) patients receiving resection of primary tumor and/or hepatic metastases, 12 patients receiving non-surgical locoregional interventions (NSLRIs), and 22 patients receiving certain kind of STs. Median overall survival (OS) was 20.0 months (95% confidence interval [CI]: 8.9-31.1 months) and survival rates were 62.6%, 30.1%, and 19.8%, at 1, 3, and 5 years, respectively. The median OS was 9.0 months (95%CI: 3.3-14.7 months) for patients receiving only STs (n = 6), 19 months (95%CI: 1.3-36.8 months) for patients receiving LT followed by STs (n = 16), and 101 months (95%CI: 0.0-210.2 months) for patients receiving only LT (n = 12). Moreover, compared with those receiving only ST or best supportive care, patients given certain types of LTs had higher rates of symptom alleviation (3/8 versus 20/23). On univariate analysis, positive prognostic factors of survival were pancreatic primary tumor (P = 0.013), normal total bilirubin level (P = 0.035), receiving surgery (P = 0.034), receiving NSLRI (P = 0.014), and sum of diameters of remnant tumor < 5 cm (P = 0.008). On multivariate analyses, pancreatic primary tumor (P = 0.015), normal total bilirubin level (P = 0.002), and sum of diameters of remnant tumor < 5 cm (P = 0.001) remained to be independent prognostic factors.For patients with G3 GEP NET liver metastases, aggressive LTs may improve clinical outcomes. Larger studies with prospective design are warranted to consolidate these results, and to discover the most appropriate seletion criteria for patients to undergo different kinds of aggressive LTs and to find the most effective combinations, with or without ST.
3级(G3)胃肠胰(GEP)神经内分泌肿瘤(NETs)较为罕见,目前尚无专门针对G3 GEP NETs肝转移患者的报道。2004年1月至2014年1月,我们从中国3家肝胆中心回顾性筛选出36例接受保守治疗的G3 GEP NETs肝转移患者,分析其临床特征和治疗结果。分别采用或联合应用积极的局部区域治疗(LT,包括减瘤手术、射频消融和肝动脉介入治疗)和全身治疗(ST),26例(72%)患者接受了原发肿瘤和/或肝转移灶切除,12例患者接受了非手术局部区域干预(NSLRI),22例患者接受了某种形式的ST。中位总生存期(OS)为20.0个月(95%置信区间[CI]:8.9 - 31.1个月),1年、3年和5年生存率分别为62.6%、30.1%和19.8%。仅接受ST的患者(n = 6)中位OS为9.0个月(95%CI:3.3 - 14.7个月),接受LT后再接受ST的患者(n = 16)中位OS为19个月(95%CI:1.3 - 36.8个月),仅接受LT的患者(n = 12)中位OS为101个月(95%CI:0.0 - 210.2个月)。此外,与仅接受ST或最佳支持治疗的患者相比,接受某些类型LT的患者症状缓解率更高(3/8对20/23)。单因素分析显示,生存的阳性预后因素包括胰腺原发肿瘤(P = 0.013)、总胆红素水平正常(P = 0.035)、接受手术(P = 0.034)、接受NSLRI(P = 0.014)以及残余肿瘤直径总和<5 cm(P = 0.008)。多因素分析显示,胰腺原发肿瘤(P = 0.015)、总胆红素水平正常(P = 0.002)以及残余肿瘤直径总和<5 cm(P = 0.001)仍然是独立的预后因素。对于G3 GEP NETs肝转移患者,积极的LT可能改善临床结局。有必要开展更大规模的前瞻性研究来巩固这些结果,确定患者接受不同类型积极LT的最合适选择标准,并找到最有效的联合治疗方案,无论是否联合ST。