Han Xu, Xu Xuefeng, Ma Hongyun, Ji Yuan, Wang Dansong, Kuang Tiantao, Wu Wenchuan, Song Bin, Li Gang, Jin Gang, Lou Wenhui
Department of Pancreatic SurgeryZhongshan Hospital, Fudan University, Shanghai, China.
Department of Pancreatic SurgeryChanghai Hospital, Second Military Medical University, Shanghai, China.
Endocr Connect. 2018 Feb;7(2):355-363. doi: 10.1530/EC-17-0388.
Emerging evidence suggests G3 pancreatic neuroendocrine neoplasms (pNENs) present heterogeneous morphology and biology. The 2017 WHO classification has introduced a new category of well-differentiated pancreatic neuroendocrine tumors (WD-pNETs) G3, compared with poorly differentiated pancreatic neuroendocrine carcinomas (PD-pNECs) G3. We aim to analysis the demographics and outcomes of patients with resectable 2017 WHO G3 pNENs to facilitate the distinction between two entities.
The multi-institutional retrospective cohort involving 57 surgically treated patients affected by 2017 WHO G3 pNENs were morphologically identified and clinically analyzed. Patients having WD-pNETs G3 and those having PD-pNECs G3 were compared.
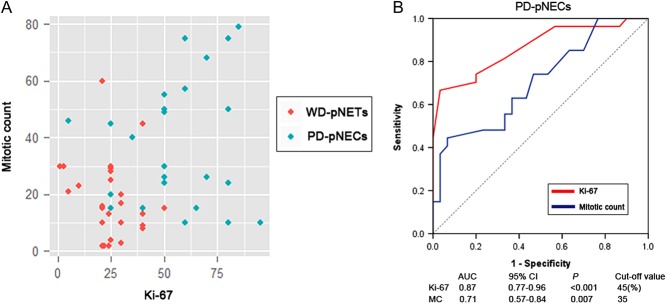
Thirty patients had WD-pNETs and 27 patients had PD-pNECs. The distributions of Ki-67 and mitotic count in patients with PD-pNECs or WD-pNETs showed remarkable disparities. ROC indicated cut-off value of Ki-67 was 45. PD-pNECs were more common in patients with elevated Ki-67 and mitotic count, advanced AJCC TNM stage, vascular invasion, regional lymph-node metastases, elevated NSE and decreased CgA levels compared with WD-pNETs ( < 0.05). The association between 2017 WHO G3 grade and TTR was statistically significant ( < 0.05). Univariate analysis indicated OS rates were associated with morphologic differentiation (WD-pNETs vs PD-pNECs), Ki-67, TNM staging, synchronous distant metastases, initial treatments, vascular invasion, regional lymph nodes metastases, mitotic count and age ( < 0.05). Multivariate analyses illustrated Ki-67, differentiation, TNM staging and vascular invasion were independent predictors ( < 0.05).
PD-pNECs G3 presented malignant biological behavior and dismal outcome compared with WD-pNETs G3. These findings challenge 2010 WHO classification and suggest the categorization can be improved by refined tumor grading.
新出现的证据表明,G3级胰腺神经内分泌肿瘤(pNENs)呈现出异质性的形态和生物学特性。2017年世界卫生组织(WHO)分类引入了一类新的高分化胰腺神经内分泌肿瘤(WD-pNETs)G3,与低分化胰腺神经内分泌癌(PD-pNECs)G3相区分。我们旨在分析2017年WHO G3级可切除pNENs患者的人口统计学特征和预后,以促进这两种实体之间的区分。
对57例接受手术治疗的2017年WHO G3级pNENs患者进行多机构回顾性队列研究,进行形态学鉴定和临床分析。比较高分化胰腺神经内分泌肿瘤(WD-pNETs)G3患者和低分化胰腺神经内分泌癌(PD-pNECs)G3患者。
30例患者为WD-pNETs,27例患者为PD-pNECs。PD-pNECs或WD-pNETs患者的Ki-67和有丝分裂计数分布存在显著差异。ROC曲线表明Ki-67的临界值为45。与WD-pNETs相比,PD-pNECs在Ki-67和有丝分裂计数升高、美国癌症联合委员会(AJCC)TNM分期晚期、血管侵犯、区域淋巴结转移、神经元特异性烯醇化酶(NSE)升高和嗜铬粒蛋白A(CgA)水平降低的患者中更常见(P<0.05)。2017年WHO G3级与无进展生存期(TTR)之间的关联具有统计学意义(P<0.05)。单因素分析表明,总生存期(OS)率与形态学分化(WD-pNETs与PD-pNECs)、Ki-67、TNM分期、同步远处转移、初始治疗、血管侵犯、区域淋巴结转移、有丝分裂计数和年龄相关(P<0.05)。多因素分析表明,Ki-67、分化、TNM分期和血管侵犯是独立的预测因素(P<0.05)。
与WD-pNETs G3相比,PD-pNECs G3表现出恶性生物学行为和不良预后。这些发现对2010年WHO分类提出了挑战,并表明通过完善肿瘤分级可以改进分类。