Browning David J, Lee Chong
Department of Ophthalmology, Charlotte Eye, Ear, Nose and Throat Associates, Charlotte, NC, USA.
Clin Ophthalmol. 2015 Aug 20;9:1499-509. doi: 10.2147/OPTH.S87850. eCollection 2015.
To quantify the variability of scotomas detected by 10-2 visual field (VF) testing with a red target in patients taking hydroxychloroquine without and with retinopathy.
Retrospective review of clinical charts and VFs.
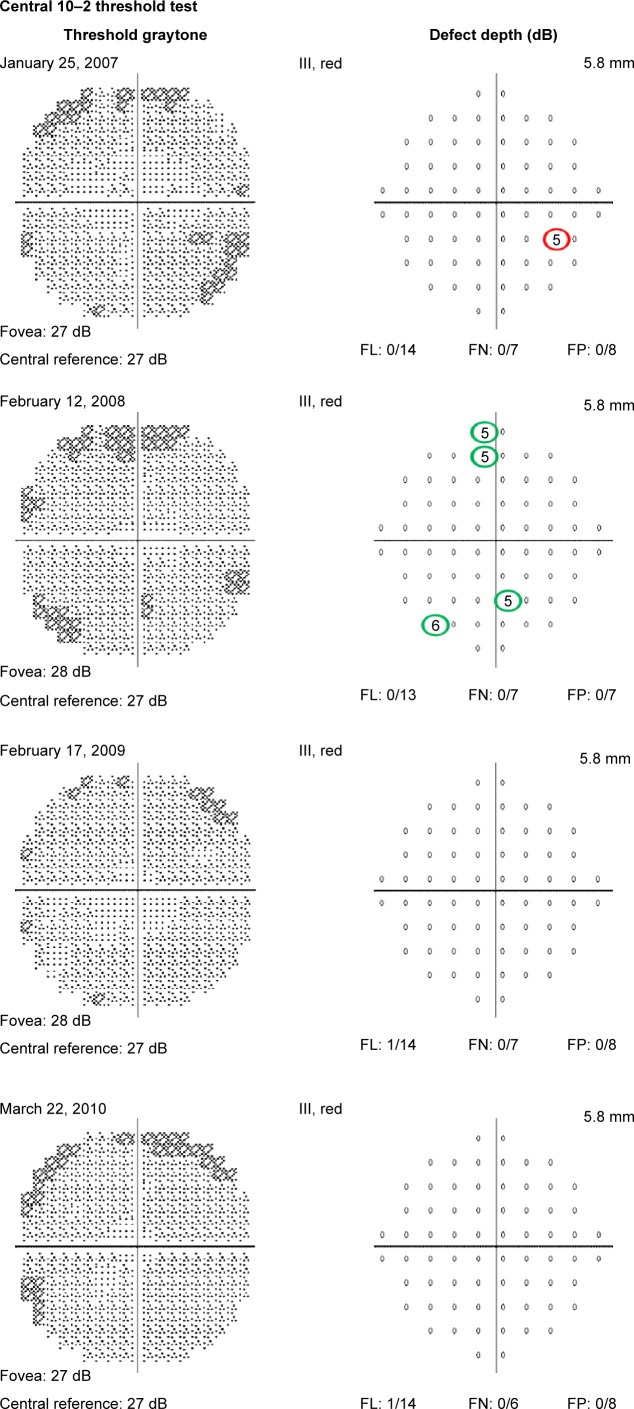
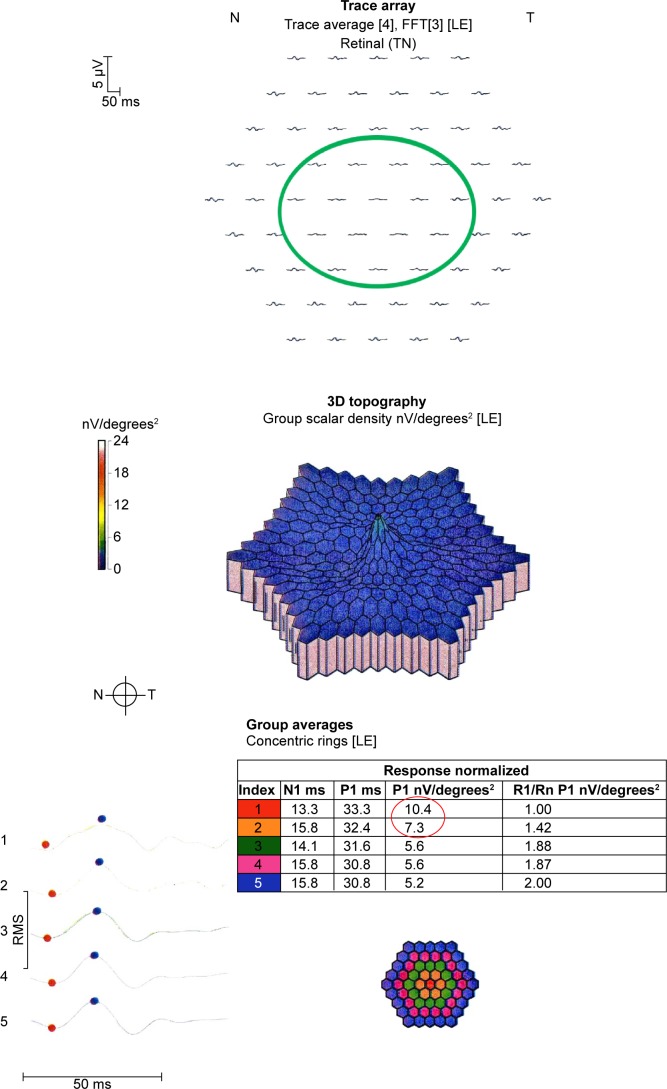
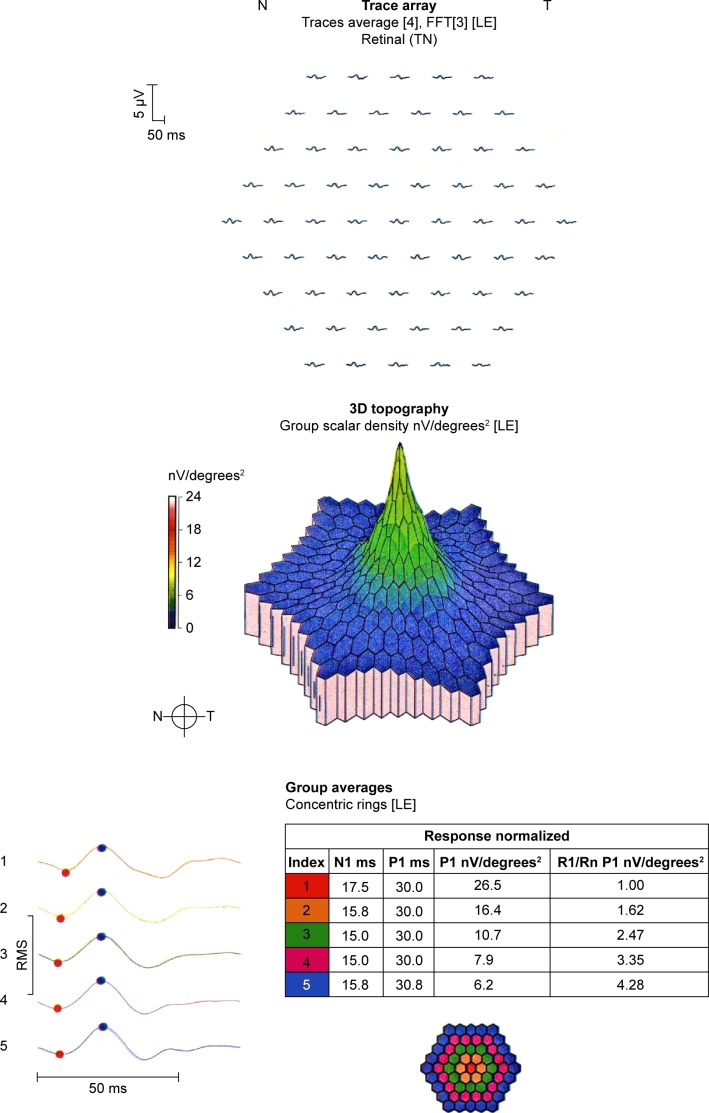
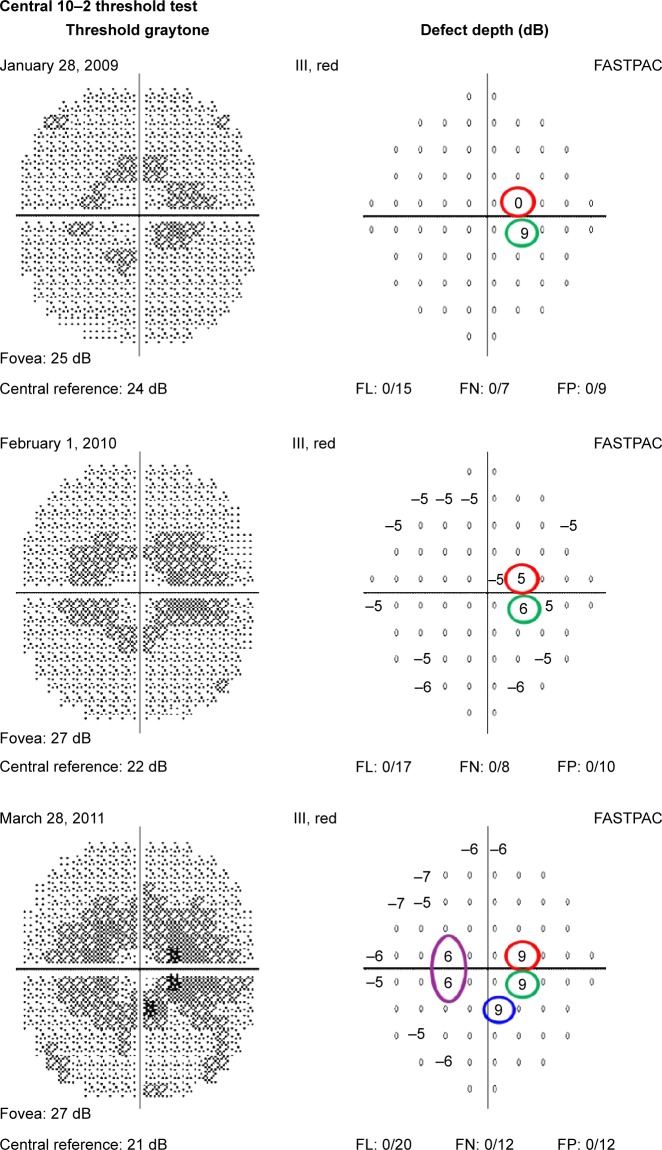
Twenty-four patients taking hydroxychloroquine without retinopathy, and eight patients taking hydroxychloroquine with retinopathy were tested in this study. Retinopathy was defined by annular scotomas on 10-2 VF testing with corroborative spectral domain optical coherence tomographic outer retinal changes and multifocal electroretinographic changes leading to cessation of hydroxychloroquine or chloroquine. Location and depth of scotoma points on 10-2 VF testing were recorded and their fates followed in serial, reliable 10-2 VFs performed with a red target over time. The main outcome measures for this study were the number of scotoma points and locations, percentage of persistent scotoma points, size of scotomas, location of scotomas, and percentage of scotomas deepening.
A median of 3, interquartile range (IQR) (2, 5), scotoma points per VF occurred in patients without retinopathy. A median of 86%, IQR (77, 100), of these resolved on the subsequent field. For patients with retinopathy, a median of 50%, IQR (46, 79), resolved, a difference compared to patients without retinopathy that was significant (P=0.0158). The median percentage of scotoma points in the zone from 2° to 8° from fixation in eyes with retinopathy was 72%, IQR (54, 100), compared to 49%, IQR (40, 54), in eyes without retinopathy (P=0.0069). The number of persistent scotoma locations at the last visit was higher in eyes with retinopathy: 3, IQR (1, 3), versus 0, IQR (0, 1), in patients without retinopathy, P=0.0156.
Point scotomas are common and variable in 10-2 VF testing with a red target for hydroxychloroquine retinopathy in subjects without retinopathy. Scotoma points in eyes with retinopathy are less variable. The annular zone 2°-8° from fixation was useful for distinguishing the significance of scotoma points. Discriminating eyes with retinopathy from eyes without retinopathy is probably easier using the 10-2 VF with a white target than a red target.
量化在服用羟氯喹且未发生视网膜病变以及已发生视网膜病变的患者中,使用红色视标进行10-2视野(VF)检测所发现的暗点的变异性。
对临床病历和视野检测结果进行回顾性分析。
本研究检测了24例服用羟氯喹但未发生视网膜病变的患者以及8例服用羟氯喹且已发生视网膜病变的患者。视网膜病变的定义为10-2视野检测出现环形暗点,并伴有辅助性光谱域光学相干断层扫描显示的视网膜外层改变以及多焦视网膜电图改变,最终导致停用羟氯喹或氯喹。记录10-2视野检测中暗点的位置和深度,并在随时间进行的一系列可靠的使用红色视标的10-2视野检测中跟踪其变化情况。本研究的主要结局指标包括暗点的数量和位置、持续性暗点的百分比、暗点大小、暗点位置以及暗点加深的百分比。
未发生视网膜病变的患者每次视野检测中暗点数量的中位数为3个,四分位间距(IQR)为(2,5)个。其中86%(IQR为77%,100%)的暗点在随后的视野检测中消失。对于发生视网膜病变的患者,暗点消失的中位数为50%(IQR为46%,79%),与未发生视网膜病变的患者相比差异有统计学意义(P = 0.0158)。发生视网膜病变的眼睛中,距注视点2°至8°区域内暗点的中位数百分比为72%(IQR为54%,100%),而未发生视网膜病变的眼睛中该比例为49%(IQR为40%,54%)(P = 0.0069)。在最后一次就诊时,发生视网膜病变的眼睛中持续性暗点位置的数量更高:中位数为3个(IQR为1,3),而未发生视网膜病变的患者为0个(IQR为0,1),P = 0.0156。
在未发生视网膜病变的受试者中,使用红色视标进行10-2视野检测时,点状暗点常见且具有变异性。发生视网膜病变的眼睛中的暗点变异性较小。距注视点2° - 8°的环形区域有助于区分暗点的意义。使用白色视标进行10-2视野检测可能比使用红色视标更容易区分发生视网膜病变的眼睛和未发生视网膜病变的眼睛。