Verma Subodh, Eikelboom John W, Nidorf Stefan M, Al-Omran Mohammed, Gupta Nandini, Teoh Hwee, Friedrich Jan O
Division of Cardiac Surgery, Keenan Research Centre for Biomedical Science and Li Ka Shing Knowledge Institute of St. Michael's Hospital, Toronto, ON, Canada.
Department of Surgery, Keenan Research Centre for Biomedical Science and Li Ka Shing Knowledge Institute of St. Michael's Hospital, Toronto, ON, Canada.
BMC Cardiovasc Disord. 2015 Aug 29;15:96. doi: 10.1186/s12872-015-0068-3.
Colchicine has unique anti-inflammatory properties that may be beneficial in various cardiovascular conditions. This systematic review and meta-analysis of randomized controlled trials (RCTs) examines this issue.
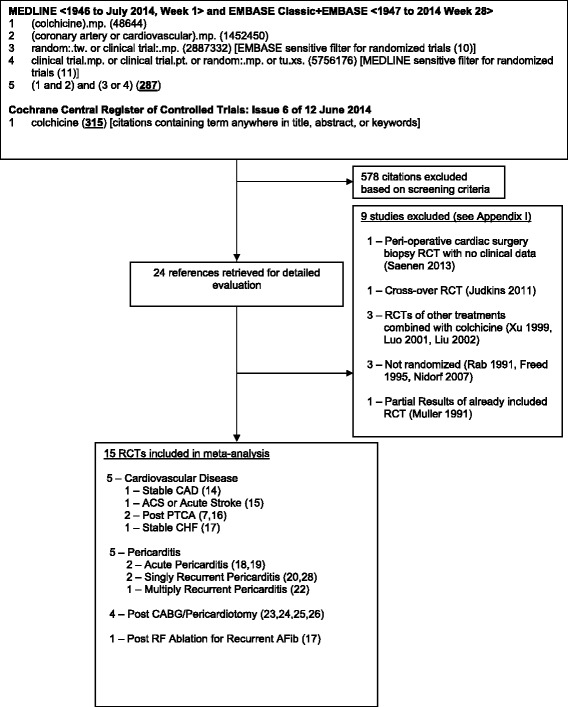
We searched MEDLINE, EMBASE, and the Cochrane Database from inception to June 2014 for RCTs using colchicine in adult patients with cardiac diseases. Results were pooled using random effects.
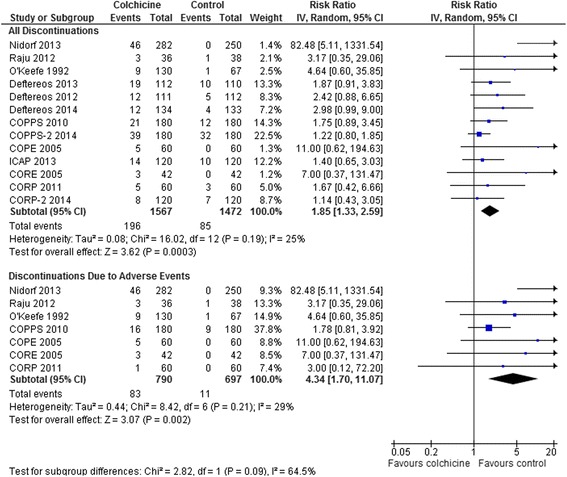
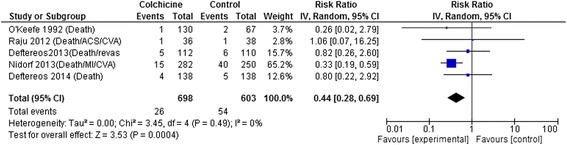
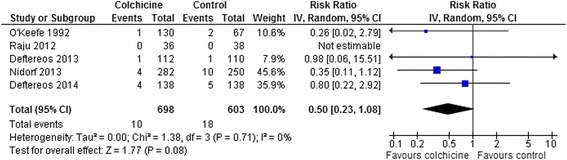
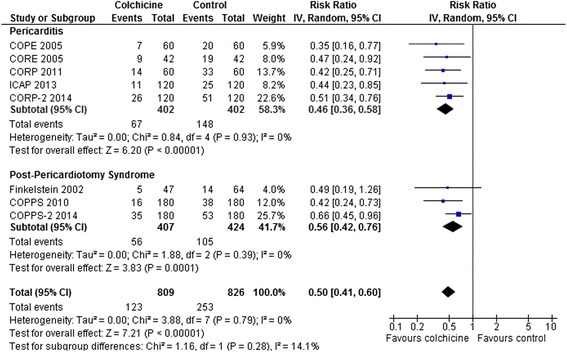
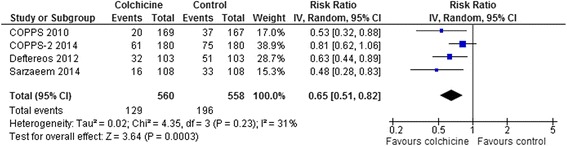
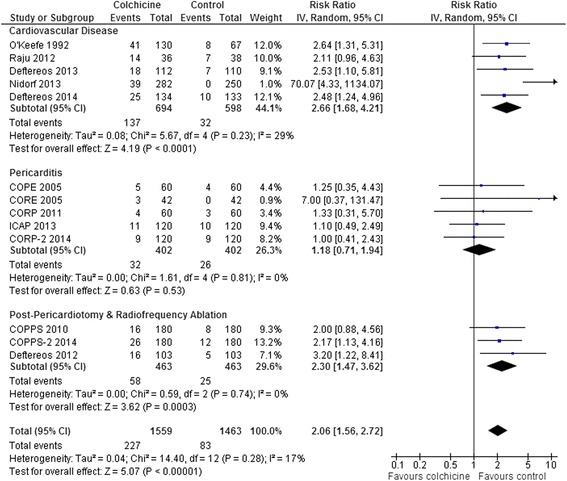
15 RCTs (n = 3431 patients, median treatment 3 and follow-up 15 months) were included. All but 2 used colchicine 1 mg/day. In 5 trials, n = 1301) at risk for cardiovascular disease (coronary artery disease, acute coronary syndrome or stroke, post-angioplasty [2 RCTs], or congestive heart failure), colchicine reduced composite cardiovascular outcomes by ~60 % (risk ratio [RR] 0.44, 95 % confidence interval [CI] 0.28-0.69, p = 0.0004; I(2) = 0 %) and showed a trend towards lower all-cause mortality (RR 0.50, 95 % CI 0.23-1.08, p = 0.08; I(2) = 0 %). In pericarditis or post-cardiotomy, colchicine decreased recurrent pericarditis or post-pericardiotomy syndrome (RR 0.50, 95 % CI 0.41-0.60, p < 0.0001; I(2) = 0 %; 8 RCTs, n = 1635), and post-pericardiotomy or ablation induced atrial fibrillation (RR 0.65, 95 % CI 0.51-0.82, p = 0.0003; I(2) = 31 %; 4 RCTs, n = 1118). The most common adverse event was diarrhea. Treatment discontinuation overall and due to adverse events (RR 4.34, 95 % CI 1.70-11.07, p = 0.002; I(2) = 29 %; 7 RCTs, 83/790 [10.5 %] vs. 11/697 [1.6 %]) was higher in colchicine-assigned patients.
Current RCT data suggests that colchicine may reduce the composite rate of cardiovascular adverse outcomes in a range of patients with established cardiovascular disease. Furthermore, colchicine reduces rates of recurrent pericarditis, post-pericardiotomy syndrome, and peri-procedural atrial fibrillation following cardiac surgery. Further RCTs evaluating the potential of colchicine for secondary prevention of cardiovascular events would be of interest.
秋水仙碱具有独特的抗炎特性,可能对多种心血管疾病有益。本随机对照试验(RCT)的系统评价和荟萃分析探讨了这一问题。
我们检索了MEDLINE、EMBASE和Cochrane数据库,从建库至2014年6月,查找在成年心脏病患者中使用秋水仙碱的RCT。采用随机效应模型合并结果。
纳入15项RCT(n = 3431例患者,中位治疗时间3个月,中位随访时间15个月)。除2项研究外,其余均使用1毫克/天的秋水仙碱。在5项试验中(n = 1301),针对有心血管疾病风险的患者(冠状动脉疾病、急性冠状动脉综合征或中风、血管成形术后[2项RCT]或充血性心力衰竭),秋水仙碱使复合心血管结局降低约60%(风险比[RR] 0.44,95%置信区间[CI] 0.28 - 0.69,p = 0.0004;I² = 0%),且全因死亡率有降低趋势(RR 0.50,95% CI 0.23 - 1.08,p = 0.08;I² = 0%)。在心包炎或心脏手术后,秋水仙碱降低了复发性心包炎或心脏术后综合征的发生率(RR 0.50,95% CI 0.41 - 0.60,p < 0.0001;I² = 0%;8项RCT,n = 1635),以及心脏术后或消融术后房颤的发生率(RR 0.65,95% CI 0.51 - 0.82,p = 0.0003;I² = 31%;4项RCT,n = 1118)。最常见的不良事件是腹泻。总体上以及因不良事件导致的治疗中断率(RR 4.34,95% CI 1.70 - 11.07,p = 0.002;I² = 29%;7项RCT,83/790 [10.5%] 对比11/697 [1.6%])在使用秋水仙碱的患者中更高。
目前的RCT数据表明,秋水仙碱可能降低一系列已确诊心血管疾病患者的心血管不良结局复合发生率。此外,秋水仙碱可降低心脏手术后复发性心包炎、心脏术后综合征及围手术期房颤的发生率。进一步评估秋水仙碱在心血管事件二级预防方面潜力的RCT将很有意义。