Marijon Eloi, Leclercq Christophe, Narayanan Kumar, Boveda Serge, Klug Didier, Lacaze-Gadonneix Jonathan, Defaye Pascal, Jacob Sophie, Piot Olivier, Deharo Jean-Claude, Perier Marie-Cecile, Mulak Genevieve, Hermida Jean-Sylvain, Milliez Paul, Gras Daniel, Cesari Olivier, Hidden-Lucet Françoise, Anselme Frederic, Chevalier Philippe, Maury Philippe, Sadoul Nicolas, Bordachar Pierre, Cazeau Serge, Chauvin Michel, Empana Jean-Philippe, Jouven Xavier, Daubert Jean-Claude, Le Heuzey Jean-Yves
Cardiology Department, European Georges Pompidou Hospital, Paris, France Paris Descartes University, Paris, France Paris Cardiovascular Research Centre, Paris, France.
Pontchaillou University Hospital and INSERM 1099, CIC-IT 804 Rennes, France.
Eur Heart J. 2015 Nov 1;36(41):2767-76. doi: 10.1093/eurheartj/ehv455. Epub 2015 Sep 1.
The choice of resynchronization therapy between with (CRT-D) and without (CRT-P) a defibrillator remains a contentious issue. Cause-of-death analysis among CRT-P, compared with CRT-D, patients could help evaluate the extent to which CRT-P patients would have additionally benefited from a defibrillator in a daily clinical practice.
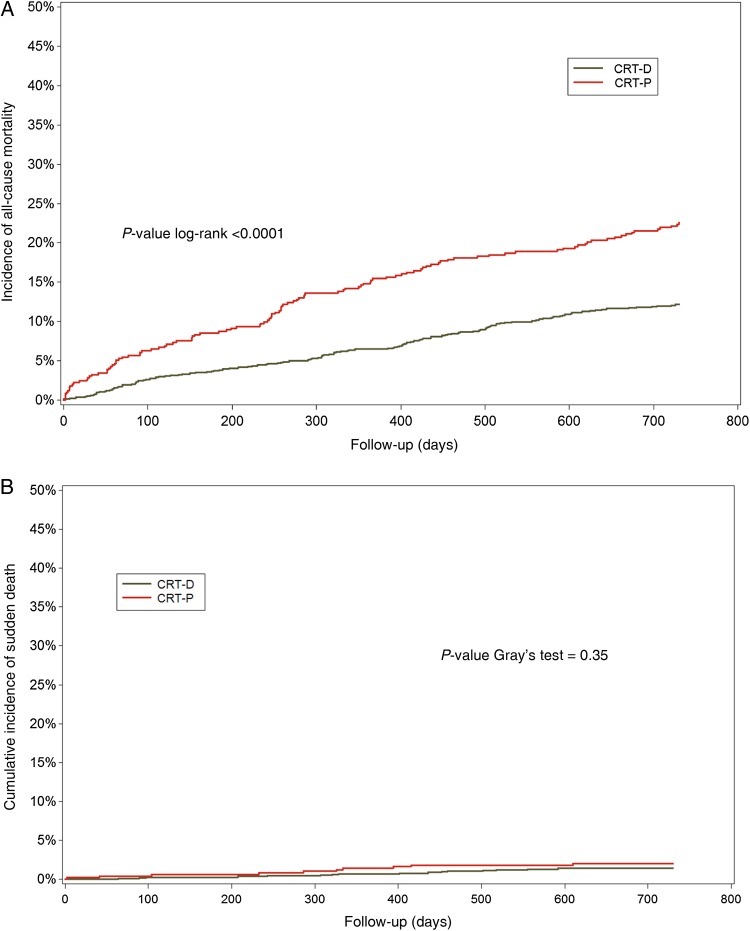
A total of 1705 consecutive patients implanted with a CRT (CRT-P: 535 and CRT-D: 1170) between 2008 and 2010 were enrolled in CeRtiTuDe, a multicentric prospective follow-up cohort study, with specific adjudication for causes of death at 2 years. Patients with CRT-P compared with CRT-D were older (P < 0.0001), less often male (P < 0.0001), more symptomatic (P = 0.0005), with less coronary artery disease (P = 0.003), wider QRS (P = 0.002), more atrial fibrillation (P < 0.0001), and more co-morbidities (P = 0.04). At 2-year follow-up, the annual overall mortality rate was 83.80 [95% confidence interval (CI) 73.41-94.19] per 1000 person-years. The crude mortality rate among CRT-P patients was double compared with CRT-D (relative risk 2.01, 95% CI 1.56-2.58). In a Cox proportional hazards regression analysis, CRT-P remained associated with increased mortality (hazard ratio 1.54, 95% CI 1.07-2.21, P = 0.0209), although other potential confounders may persist. By cause-of-death analysis, 95% of the excess mortality among CRT-P subjects was related to an increase in non-sudden death.
When compared with CRT-D patients, excess mortality in CRT-P recipients was mainly due to non-sudden death. Our findings suggest that CRT-P patients, as currently selected in routine clinical practice, would not potentially benefit with the addition of a defibrillator.
在有除颤器(CRT-D)和无除颤器(CRT-P)的心脏再同步治疗之间进行选择仍然是一个有争议的问题。对CRT-P患者与CRT-D患者进行死因分析,有助于评估在日常临床实践中CRT-P患者额外使用除颤器可能带来的获益程度。
在2008年至2010年期间,共有1705例连续植入心脏再同步治疗设备的患者(CRT-P:535例,CRT-D:1170例)纳入了CeRtiTuDe研究,这是一项多中心前瞻性随访队列研究,对2年时的死因进行了专门判定。与CRT-D患者相比,CRT-P患者年龄更大(P<0.0001),男性比例更低(P<0.0001),症状更明显(P = 0.0005),冠心病更少(P = 0.003),QRS波更宽(P = 0.002),房颤更多(P<0.0001),合并症更多(P = 0.04)。在2年随访时,年总死亡率为每1000人年83.80例[95%置信区间(CI)73.41 - 94.19]。CRT-P患者的粗死亡率是CRT-D患者的两倍(相对风险2.01,95%CI 1.56 - 2.58)。在Cox比例风险回归分析中,CRT-P仍然与死亡率增加相关(风险比1.54,95%CI 1.07 - 2.21,P = 0.0209),尽管其他潜在混杂因素可能仍然存在。通过死因分析,CRT-P患者中95%的额外死亡率与非猝死增加有关。
与CRT-D患者相比,CRT-P接受者的额外死亡率主要归因于非猝死。我们的研究结果表明,按照目前常规临床实践中选择的CRT-P患者,增加除颤器可能不会带来潜在获益。