Pan Xudong, Pang Meng, Ma Aijun, Wang Kun, Zhang Zhang, Zhong Qianwei, Yang Shuna
Department of Neurology, the Affiliated Hospital of the Qingdao University, Qingdao, Shandong Province 266100, PR China.
PLoS One. 2015 Sep 3;10(9):e0136414. doi: 10.1371/journal.pone.0136414. eCollection 2015.
To investigate the association of the tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) and its receptors, osteoprotegerin (OPG) and death receptor 5 (DR5) with large-artery atherosclerosis (LAA) stroke and its prognosis.
We included patients with LAA stroke (n = 132) according to the TOAST classification system and controls (n = 60). To evaluate the extent and severity of cerebral atherosclerosis, the LAA stroke group was subdivided into 3 subgroups by number of cerebral arteries with atherosclerotic stenosis (≥50%): single, double and multiple (≥3). Plasma levels of TRAIL, OPG and DR5 were measured by ELISA. Ordinal logistic regression was used to analyze the association between the plasma levels of TRAIL, OPG, DR5 and the severity of cerebral atherosclerosis. Prognosis was determined by the Modified Rankin Scale at 3 months after stroke. Receiver operating characteristic (ROC) curve was used to evaluated TRAIL as a predictor of prognosis.
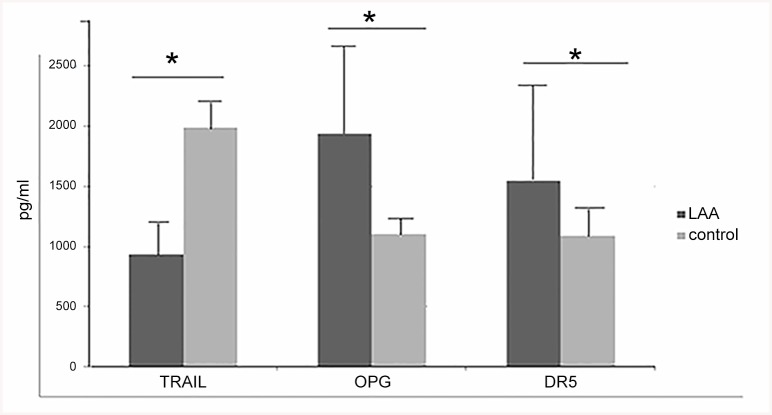
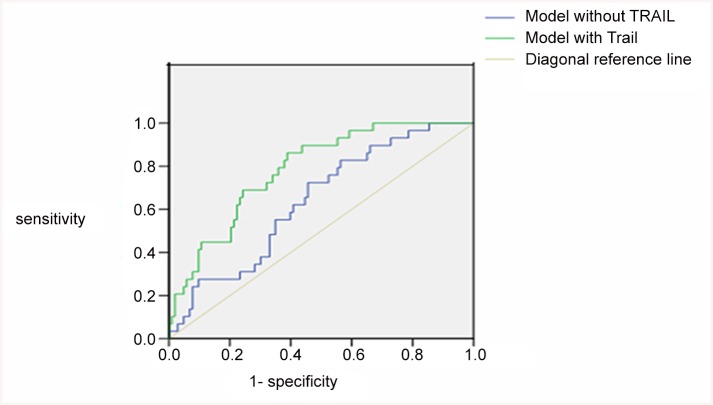
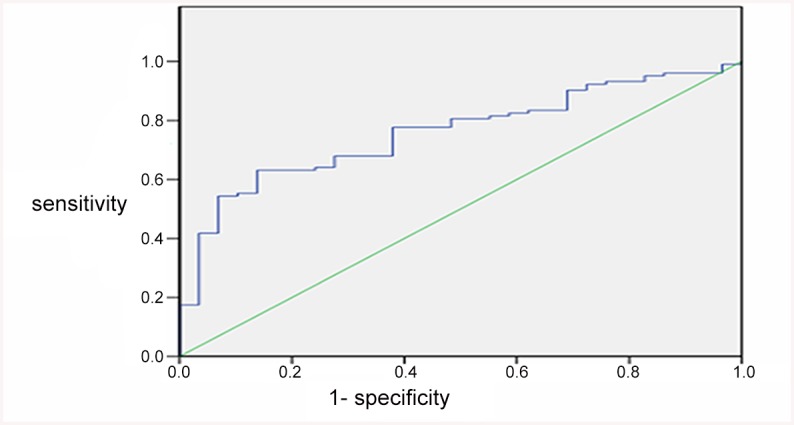
Plasma TRAIL level was significantly lower for LAA patients than controls (P<0.001), while plasma OPG and DR5 levels were higher (both P<0.001). Logistic regression analysis revealed that risk of severe cerebral atherosclerosis was reduced significantly with increased plasma level of TRAIL (OR 0.438; 95% CI 0.282-0.681; P<0.001), whereas increased with high plasma levels of OPG and DR5 (OR 2.707; 95% CI 1.702-4.302, P <0.001; OR 3.593; 95% CI 1.878-6.869, P <0.001). Plasma TRAIL level was negatively correlated with the prognosis (r = - 0.372, P <0.001). The optimal cut-off value of TRAIL for prognosis was 848.63 pg/mL. The sensitivity and specificity at this cut-off value were 63.1% and 86.2%, respectively. After adding the plasma TRAIL level into the multivariate model of ROC, the area under the ROC curve was increased from 0.639 to 0.785, but the change was not statistical significant (P = 0.146).
TRAIL and its receptors OPG and DR5 may be involved in LAA stroke and the plasma level of TRAIL may be a biomarker predicting the severity of cerebral atherosclerosis and the prognosis of LAA stroke.
探讨肿瘤坏死因子相关凋亡诱导配体(TRAIL)及其受体骨保护素(OPG)和死亡受体5(DR5)与大动脉粥样硬化(LAA)性卒中及其预后的关系。
根据TOAST分类系统纳入LAA性卒中患者(n = 132)和对照组(n = 60)。为评估脑动脉粥样硬化的范围和严重程度,LAA性卒中组根据有动脉粥样硬化狭窄(≥50%)的脑动脉数量分为3个亚组:单支、双支和多支(≥3支)。采用酶联免疫吸附测定法(ELISA)检测血浆TRAIL、OPG和DR5水平。采用有序逻辑回归分析TRAIL、OPG、DR5血浆水平与脑动脉粥样硬化严重程度之间的关系。预后通过卒中后3个月的改良Rankin量表确定。采用受试者工作特征(ROC)曲线评估TRAIL作为预后预测指标的价值。
LAA患者血浆TRAIL水平显著低于对照组(P<0.001),而血浆OPG和DR5水平较高(均P<0.001)。逻辑回归分析显示,随着血浆TRAIL水平升高,严重脑动脉粥样硬化风险显著降低(OR 0.438;95%CI 0.282 - 0.681;P<0.001),而随着血浆OPG和DR5高水平升高,风险增加(OR 2.707;95%CI 1.702 - 4.302,P <0.001;OR 3.593;95%CI 1.878 - 6.869,P <0.001)。血浆TRAIL水平与预后呈负相关(r = - 0.372,P <0.001)。TRAIL预后的最佳截断值为848.63 pg/mL。此截断值时的敏感性和特异性分别为63.1%和86.2%。将血浆TRAIL水平加入ROC多变量模型后,ROC曲线下面积从0.639增加至0.785,但变化无统计学意义(P = 0.146)。
TRAIL及其受体OPG和DR5可能参与LAA性卒中,血浆TRAIL水平可能是预测脑动脉粥样硬化严重程度和LAA性卒中预后的生物标志物。