Rata Mihaela, Collins David J, Darcy James, Messiou Christina, Tunariu Nina, Desouza Nandita, Young Helen, Leach Martin O, Orton Matthew R
CR-UK Cancer Imaging Centre, Division of Radiotherapy and Imaging, Institute of Cancer Research and Royal Marsden Hospital, London, UK.
Early Clinical Development, AstraZeneca, Macclesfield, Cheshire, UK.
Eur Radiol. 2016 Jul;26(7):1991-8. doi: 10.1007/s00330-015-4012-9. Epub 2015 Sep 18.
Pharmacokinetic (PK) modelling of dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) data requires a reliable measure of the arterial input function (AIF) to robustly characterise tumour vascular properties. This study compared repeatability and treatment-response effects of DCE-MRI-derived PK parameters using a population-averaged AIF and three patient-specific AIFs derived from pre-bolus MRI, DCE-MRI and dynamic contrast computed tomography (DC-CT) data.
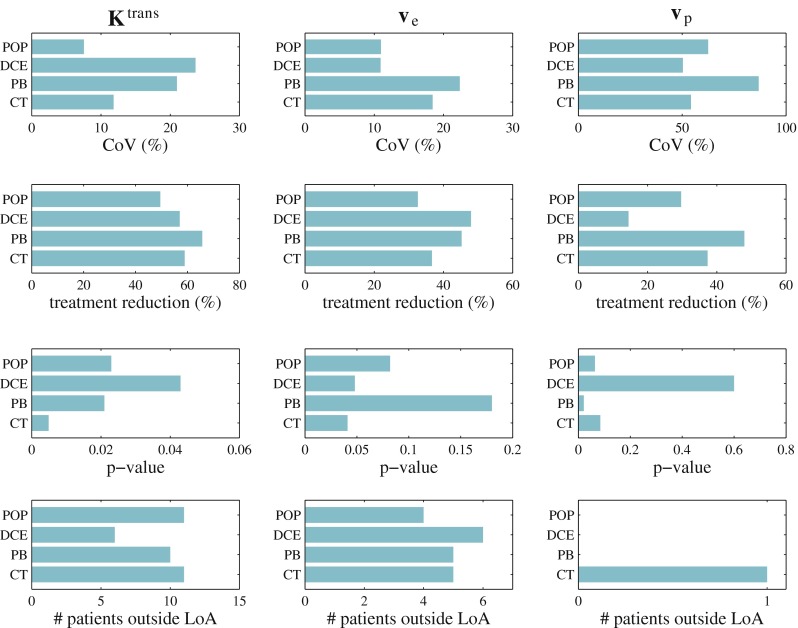
The four approaches were compared in 13 patients with abdominal metastases. Baseline repeatability [Bland-Altman statistics; coefficient of variation (CoV)], cohort percentage change and p value (paired t test) and number of patients with significant DCE-MRI parameter change post-treatment (limits of agreement) were assessed.
Individual AIFs were obtained for all 13 patients with pre-bolus MRI and DC-CT-derived AIFs, but only 10/13 patients had AIFs measurable from DCE-MRI data. The best CoV (7.5 %) of the transfer coefficient between blood plasma and extravascular extracellular space (K (trans)) was obtained using a population-averaged AIF. All four AIF methods detected significant treatment changes: the most significant was the DC-CT-derived AIF. The population-based AIF was similar to or better than the pre-bolus and DCE-MRI-derived AIFs.
A population-based AIF is the recommended approach for measuring cohort and individual effects since it has the best repeatability and none of the PK parameters derived using measured AIFs demonstrated an improvement in treatment sensitivity.
• Pharmacokinetic modelling of DCE-MRI data requires a reliable measure of AIF. • Individual MRI-DCE-derived AIFs cannot reliably be extracted from patients. • All four AIF methods detected significant K (trans) changes after treatment. • A population-based AIF can be recommended for measuring cohort treatment responses in trials.
动态对比增强磁共振成像(DCE-MRI)数据的药代动力学(PK)建模需要可靠的动脉输入函数(AIF)测量值,以稳健地表征肿瘤血管特性。本研究比较了使用群体平均AIF以及从团注前MRI、DCE-MRI和动态对比计算机断层扫描(DC-CT)数据得出的三种患者特异性AIF时,DCE-MRI衍生的PK参数的可重复性和治疗反应效果。
在13例腹部转移患者中比较了这四种方法。评估了基线重复性[布兰德-奥特曼统计量;变异系数(CoV)]、队列百分比变化和p值(配对t检验)以及治疗后DCE-MRI参数有显著变化的患者数量(一致性界限)。
使用团注前MRI和DC-CT衍生的AIF为所有13例患者获得了个体AIF,但只有10/13例患者的AIF可从DCE-MRI数据中测量得到。使用群体平均AIF时,血浆与血管外细胞外间隙之间的转运系数(K(trans))的最佳CoV为7.5%。所有四种AIF方法均检测到显著的治疗变化:最显著的是DC-CT衍生AIF。基于群体平均的AIF与团注前和DCE-MRI衍生的AIF相似或更好。
基于群体平均的AIF是测量队列和个体效应的推荐方法,因为它具有最佳的可重复性,并且使用测量得到的AIF得出的PK参数均未显示出治疗敏感性的提高。
• DCE-MRI数据的药代动力学建模需要可靠的AIF测量值。• 无法从患者中可靠地提取个体MRI-DCE衍生的AIF。• 所有四种AIF方法均检测到治疗后K(trans)有显著变化。• 基于群体平均的AIF可推荐用于在试验中测量队列治疗反应。