Williams Bryan, MacDonald Thomas M, Morant Steve, Webb David J, Sever Peter, McInnes Gordon, Ford Ian, Cruickshank J Kennedy, Caulfield Mark J, Salsbury Jackie, Mackenzie Isla, Padmanabhan Sandosh, Brown Morris J
Institute of Cardiovascular Sciences University College London and National Institute for Health Research (NIHR) UCL/UCL Hospitals Biomedical Research Centre, London, UK.
Medicines Monitoring Unit, Medical Research Institute, University of Dundee, Dundee, UK.
Lancet. 2015 Nov 21;386(10008):2059-2068. doi: 10.1016/S0140-6736(15)00257-3. Epub 2015 Sep 20.
Optimal drug treatment for patients with resistant hypertension is undefined. We aimed to test the hypotheses that resistant hypertension is most often caused by excessive sodium retention, and that spironolactone would therefore be superior to non-diuretic add-on drugs at lowering blood pressure.
In this double-blind, placebo-controlled, crossover trial, we enrolled patients aged 18-79 years with seated clinic systolic blood pressure 140 mm Hg or greater (or ≥135 mm Hg for patients with diabetes) and home systolic blood pressure (18 readings over 4 days) 130 mm Hg or greater, despite treatment for at least 3 months with maximally tolerated doses of three drugs, from 12 secondary and two primary care sites in the UK. Patients rotated, in a preassigned, randomised order, through 12 weeks of once daily treatment with each of spironolactone (25-50 mg), bisoprolol (5-10 mg), doxazosin modified release (4-8 mg), and placebo, in addition to their baseline blood pressure drugs. Random assignment was done via a central computer system. Investigators and patients were masked to the identity of drugs, and to their sequence allocation. The dose was doubled after 6 weeks of each cycle. The hierarchical primary endpoints were the difference in averaged home systolic blood pressure between spironolactone and placebo, followed (if significant) by the difference in home systolic blood pressure between spironolactone and the average of the other two active drugs, followed by the difference in home systolic blood pressure between spironolactone and each of the other two drugs. Analysis was by intention to treat. The trial is registered with EudraCT number 2008-007149-30, and ClinicalTrials.gov number, NCT02369081.
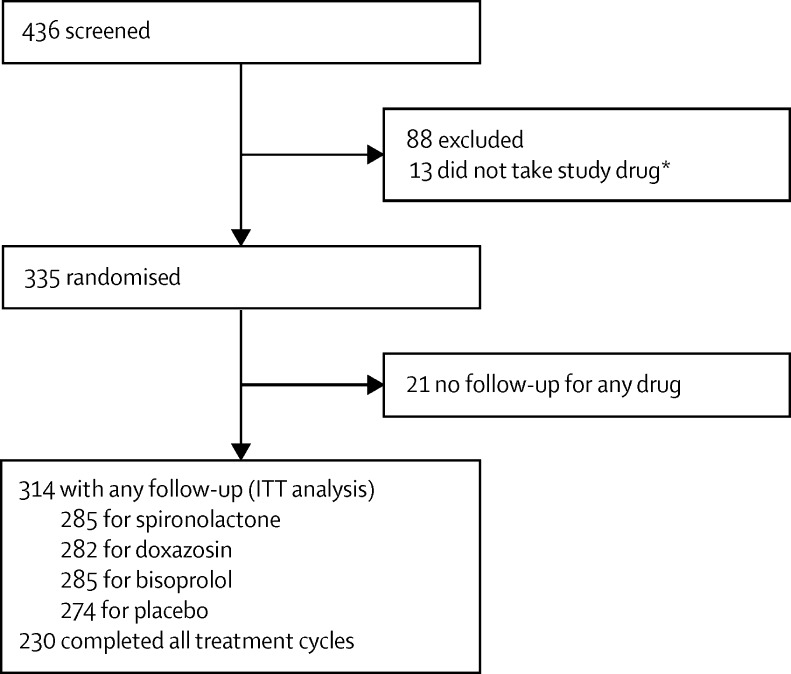
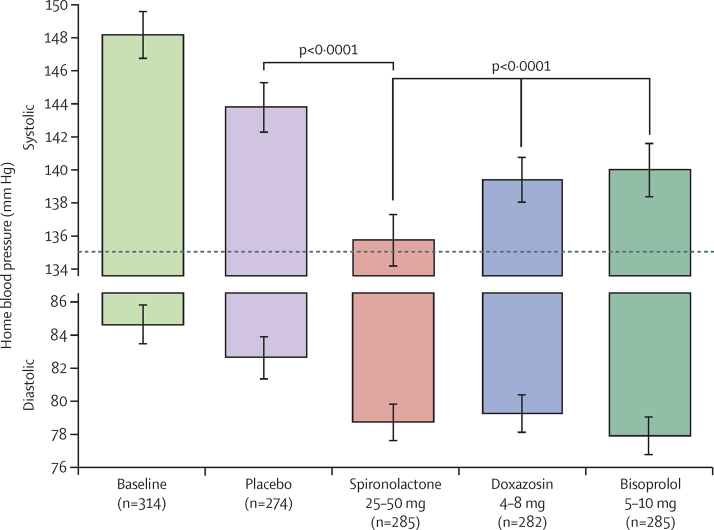
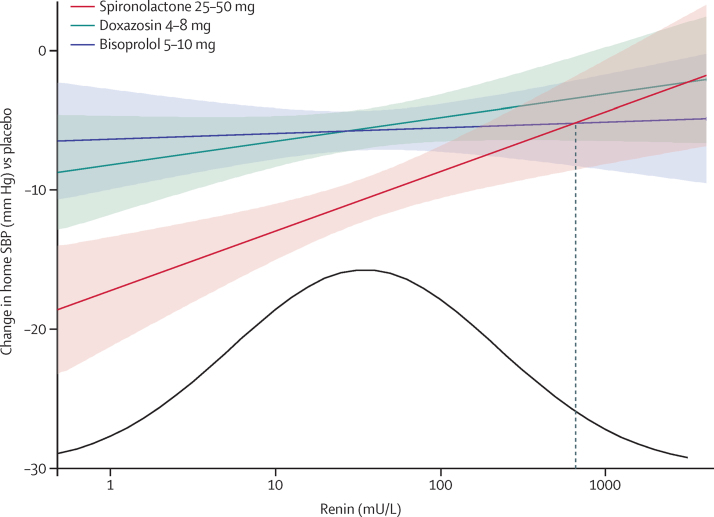
Between May 15, 2009, and July 8, 2014, we screened 436 patients, of whom 335 were randomly assigned. After 21 were excluded, 285 patients received spironolactone, 282 doxazosin, 285 bisoprolol, and 274 placebo; 230 patients completed all treatment cycles. The average reduction in home systolic blood pressure by spironolactone was superior to placebo (-8·70 mm Hg [95% CI -9·72 to -7·69]; p<0·0001), superior to the mean of the other two active treatments (doxazosin and bisoprolol; -4·26 [-5·13 to -3·38]; p<0·0001), and superior when compared with the individual treatments; versus doxazosin (-4·03 [-5·04 to -3·02]; p<0·0001) and versus bisoprolol (-4·48 [-5·50 to -3·46]; p<0·0001). Spironolactone was the most effective blood pressure-lowering treatment, throughout the distribution of baseline plasma renin; but its margin of superiority and likelihood of being the best drug for the individual patient were many-fold greater in the lower than higher ends of the distribution. All treatments were well tolerated. In six of the 285 patients who received spironolactone, serum potassium exceeded 6·0 mmol/L on one occasion.
Spironolactone was the most effective add-on drug for the treatment of resistant hypertension. The superiority of spironolactone supports a primary role of sodium retention in this condition.
The British Heart Foundation and National Institute for Health Research.
顽固性高血压患者的最佳药物治疗方案尚未明确。我们旨在验证以下假设:顽固性高血压最常见的病因是钠潴留过多,因此螺内酯在降低血压方面优于非利尿剂附加药物。
在这项双盲、安慰剂对照、交叉试验中,我们纳入了年龄在18 - 79岁之间的患者,这些患者在诊所坐位收缩压为140 mmHg或更高(糖尿病患者为≥135 mmHg),且家庭收缩压(4天内18次读数)为130 mmHg或更高,尽管已使用最大耐受剂量的三种药物进行了至少3个月的治疗,这些患者来自英国的12个二级医疗和2个初级医疗站点。患者按照预先指定的随机顺序,除了服用基线降压药物外,依次接受为期12周的每日一次治疗,分别使用螺内酯(25 - 50 mg)、比索洛尔(5 - 10 mg)、多沙唑嗪控释片(4 - 8 mg)和安慰剂。随机分组通过中央计算机系统进行。研究人员和患者对药物的身份及其序列分配均不知情。每个周期6周后剂量加倍。分层主要终点为螺内酯与安慰剂之间家庭收缩压平均值的差异,若有显著差异,则接着比较螺内酯与其他两种活性药物平均值之间家庭收缩压的差异,然后比较螺内酯与其他两种药物各自之间家庭收缩压的差异。分析采用意向性分析。该试验在欧洲药品管理局临床试验注册数据库(EudraCT)的注册号为2008 - 007,149 - 30,在美国国立医学图书馆临床试验注册库(ClinicalTrials.gov)的注册号为NCT02369081。
在2009年5月15日至2014年7月8日期间,我们筛选了436例患者,其中335例被随机分配。排除21例后,285例患者接受螺内酯治疗,282例接受多沙唑嗪治疗,285例接受比索洛尔治疗,274例接受安慰剂治疗;230例患者完成了所有治疗周期。螺内酯使家庭收缩压的平均降低幅度优于安慰剂(-8.70 mmHg [95%CI -9.72至-7.69];p<0.0001),优于其他两种活性治疗药物(多沙唑嗪和比索洛尔)的平均值(-4.26 [-5.13至-3.38];p<0.0001),与单独使用其他两种药物相比也更优;与多沙唑嗪相比(-4.03 [-5.04至-3.02];p<0.0001),与比索洛尔相比(-4.48 [-5.50至-3.46];p<0.0001)。在整个基线血浆肾素分布范围内,螺内酯是最有效的降压治疗药物;但其优势幅度以及成为个体患者最佳药物的可能性在分布的低端比高端大很多倍。所有治疗的耐受性均良好。在接受螺内酯治疗的285例患者中(有)6例血清钾有一次超过6.0 mmol/L。
螺内酯是治疗顽固性高血压最有效的附加药物。螺内酯的优势支持了钠潴留在此病症中的主要作用。
英国心脏基金会和英国国家卫生研究院。