Salfati Elias, Nandkeolyar Shuktika, Fortmann Stephen P, Sidney Stephen, Hlatky Mark A, Quertermous Thomas, Go Alan S, Iribarren Carlos, Herrington David M, Goldstein Benjamin A, Assimes Themistocles L
From the Department of Medicine, Stanford University School of Medicine, CA (E.S., S.P.F., M.A.H., T.Q., B.A.G., T.L.A.); Ecole Doctorale B2T, IUH, Université Paris 7, Paris, France (E.S.); Medical College of Wisconsin, Milwaukee (S.N.); Kaiser Permanente Center for Health Research, Portland, OR (S.P.F.); Kaiser Permanente Division of Research, Oakland, CA (S.S., A.S.G., C.I.); Heart and Vascular Center of Excellence, Wake Forest School of Medicine, Winston-Salem, NC (D.M.H.); and Department of Biostatistics and Bioinformatics, Duke University, Durham, NC (B.A.G.).
Circ Cardiovasc Genet. 2015 Dec;8(6):803-11. doi: 10.1161/CIRCGENETICS.114.001071. Epub 2015 Sep 28.
Recent genome-wide association studies have identified 49 single nucleotide polymorphisms associated with clinical coronary artery disease. The mechanism by which these loci influence risk remains largely unclear.
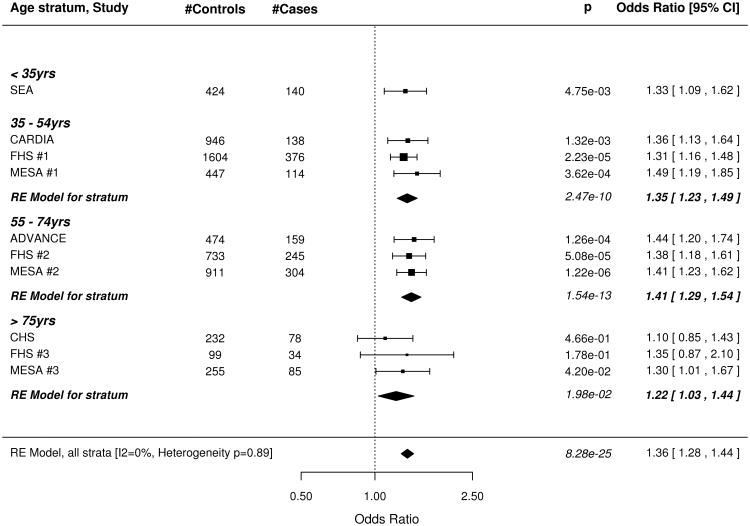
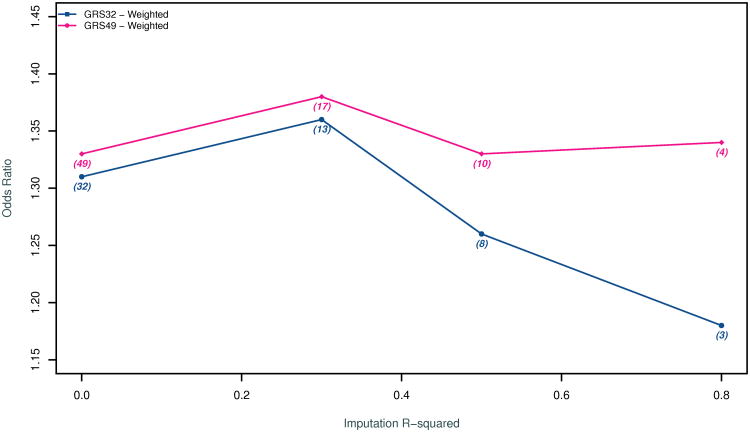
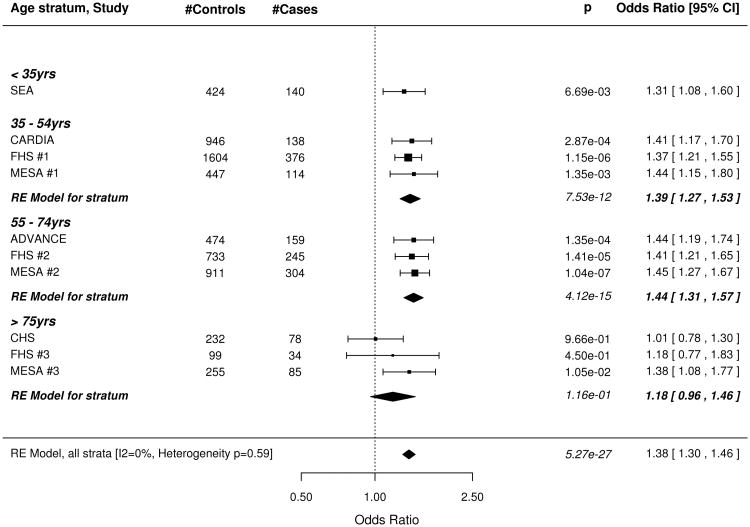
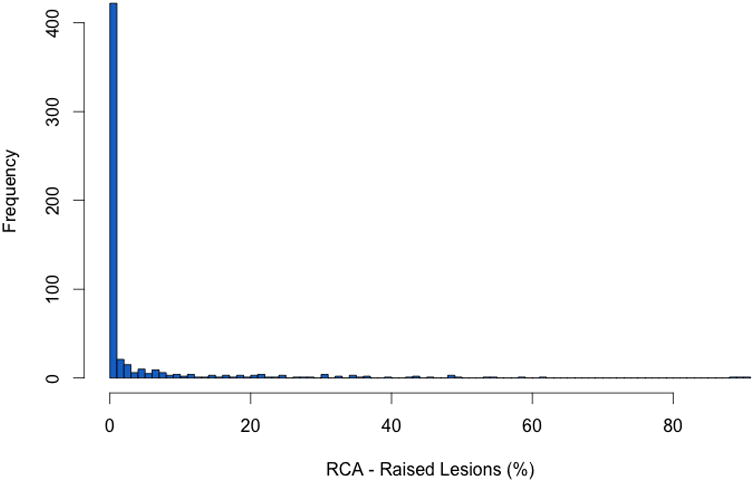
We examined the association between a genetic risk score composed of high-risk alleles at the 49 single nucleotide polymorphisms and the degree of subclinical coronary atherosclerosis in 7798 participants from 6 studies stratified into 4 age groups at the time of assessment (15-34, 35-54, 55-74, and >75 years). Atherosclerosis was quantified by staining and direct visual inspection of the right coronary artery in the youngest group and by scanning for coronary artery calcification in the remaining groups. We defined cases as subjects within the top quartile of degree of atherosclerosis in 3 groups and as subjects with a coronary artery calcium score >0 in the fourth (35-54 years) where less than one quarter had any coronary artery calcium. In our meta-analysis of all strata, we found 1-SD increase in the genetic risk score increased the risk of advanced subclinical coronary atherosclerosis by 36% (P=8.3×10(-25)). This increase in risk was significant in all 4 age groups including the youngest group where atherosclerosis consisted primarily of raised lesions without macroscopic evidence of plaque rupture or thrombosis. Results were similar when we restricted the genetic risk score to 32 single nucleotide polymorphisms not associated with traditional risk factors or when we adjusted for traditional risk factors.
A genetic risk score for clinical coronary artery disease is associated with advanced subclinical coronary atherosclerosis throughout the life-course. This association is apparent even at the earliest, uncomplicated stages of atherosclerosis.
近期全基因组关联研究已鉴定出49个与临床冠状动脉疾病相关的单核苷酸多态性。这些基因座影响风险的机制仍 largely不清楚。
我们在来自6项研究的7798名参与者中,检查了由49个单核苷酸多态性的高风险等位基因组成的遗传风险评分与亚临床冠状动脉粥样硬化程度之间的关联,这些参与者在评估时被分为4个年龄组(15 - 34岁、35 - 54岁、55 - 74岁和>75岁)。在最年轻的组中,通过对右冠状动脉进行染色和直接目视检查来量化动脉粥样硬化,在其余组中通过扫描冠状动脉钙化来量化。我们将病例定义为3个组中动脉粥样硬化程度处于最高四分位数的受试者,以及在第四个组(35 - 54岁)中冠状动脉钙评分>0的受试者,该组中不到四分之一的人有任何冠状动脉钙化。在我们对所有分层的荟萃分析中,我们发现遗传风险评分每增加1个标准差,晚期亚临床冠状动脉粥样硬化的风险增加36%(P = 8.3×10(-25))。这种风险增加在所有4个年龄组中均具有统计学意义,包括最年轻的组,该组的动脉粥样硬化主要由隆起病变组成,无斑块破裂或血栓形成的宏观证据。当我们将遗传风险评分限制在与传统风险因素无关的32个单核苷酸多态性时,或在调整传统风险因素后,结果相似。
临床冠状动脉疾病的遗传风险评分与整个生命过程中的晚期亚临床冠状动脉粥样硬化相关。即使在动脉粥样硬化最早、未并发的阶段,这种关联也很明显。