Mallhi Tauqeer Hussain, Khan Amer Hayat, Adnan Azreen Syazril, Sarriff Azmi, Khan Yusra Habib, Jummaat Fauziah
Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, University Sains Malaysia, Penang, 11800, Malaysia.
Chronic Kidney Disease Resource Centre, School of Medical Sciences, Health Campus, University Sains Malaysia, Kubang Kerain 16150, Kelantan, Malaysia.
BMC Infect Dis. 2015 Sep 30;15:399. doi: 10.1186/s12879-015-1141-3.
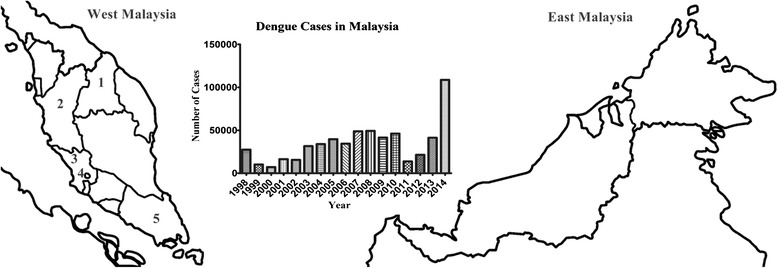
The incidence of dengue is rising steadily in Malaysia since the first major outbreak in 1973. Despite aggressive measures taken by the relevant authorities, Malaysia is still facing worsening dengue crisis over the past few years. There is an urgent need to evaluate dengue cases for better understanding of clinic-laboratory spectrum in order to combat this disease.
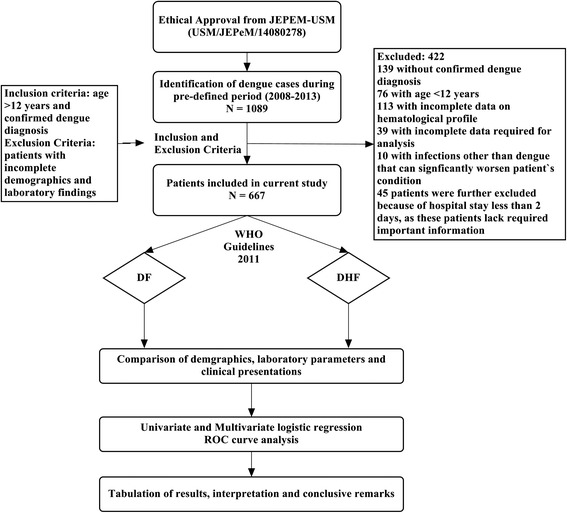
A retrospective analysis of dengue patients admitted to a tertiary care teaching hospital during the period of six years (2008 - 2013) was performed. Patient's demographics, clinical and laboratory findings were recorded via structured data collection form. Patients were categorized into dengue fever (DF) and dengue hemorrhagic fever (DHF). Appropriate statistical methods were used to compare these two groups in order to determine difference in clinico-laboratory characteristics and to identify independent risk factors of DHF.
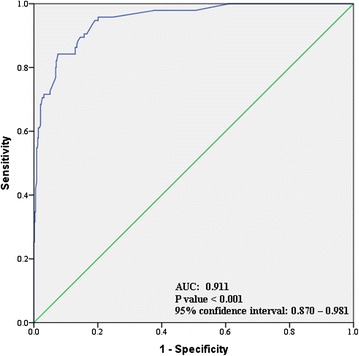
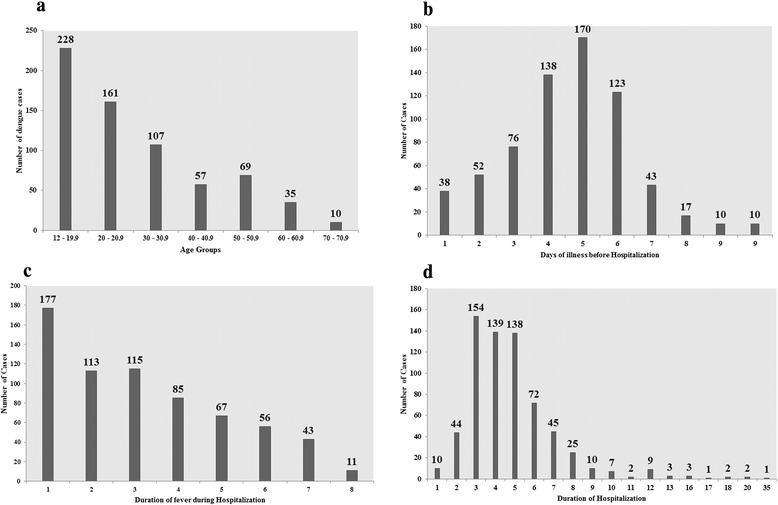
A total 667 dengue patients (30.69 ± 16.13 years; Male: 56.7 %) were reviewed. Typical manifestations of dengue like fever, myalgia, arthralgia, headache, vomiting, abdominal pain and skin rash were observed in more than 40 % patients. DHF was observed in 79 (11.8 %) cases. Skin rash, dehydration, shortness of breath, pleural effusion and thick gall bladder were more significantly (P < 0.05) associated with DHF than DF. Multivariate regression analysis demonstrated presence of age > 40 years (OR: 4.1, P < 0.001), secondary infection (OR: 2.7, P = 0.042), diabetes mellitus (OR: 2.8, P = 0.041), lethargy (OR: 3.1, P = 0.005), thick gallbladder (OR: 1.7, P = 0.029) and delayed hospitalization (OR: 2.3, P = 0.037) as independent predictors of DHF. Overall mortality was 1.2 % in our study.
Current study demonstrated that DF and DHF present significantly different clinico-laboratory profile. Older age, secondary infection, diabetes mellitus, lethargy, thick gallbladder and delayed hospitalization significantly predict DHF. Prior knowledge of expected clinical profile and predictors of DHF/DSS development would provide information to identify individuals at higher risk and on the other hand, give sufficient time to clinicians for reducing dengue related morbidity and mortality.
自1973年首次大规模登革热疫情爆发以来,马来西亚登革热发病率一直在稳步上升。尽管相关当局采取了积极措施,但在过去几年中,马来西亚仍面临着日益严重的登革热危机。迫切需要对登革热病例进行评估,以更好地了解临床实验室特征,从而抗击这种疾病。
对一家三级护理教学医院在六年期间(2008 - 2013年)收治的登革热患者进行回顾性分析。通过结构化数据收集表记录患者的人口统计学、临床和实验室检查结果。将患者分为登革热(DF)和登革出血热(DHF)。采用适当的统计方法对这两组进行比较,以确定临床实验室特征的差异,并确定DHF的独立危险因素。
共回顾了667例登革热患者(年龄30.69±16.13岁;男性:56.7%)。超过40%的患者出现了登革热的典型症状,如发热、肌痛、关节痛、头痛、呕吐、腹痛和皮疹。79例(11.8%)患者被诊断为DHF。与DF相比,皮疹、脱水、呼吸急促、胸腔积液和胆囊壁增厚与DHF的相关性更为显著(P<0.05)。多因素回归分析显示,年龄>40岁(OR:4.1,P<0.001)、二次感染(OR:2.7,P = 0.042)、糖尿病(OR:2.8,P = 0.041)、嗜睡(OR:3.1,P = 0.005)、胆囊壁增厚(OR:1.7,P = 0.029)和延迟住院(OR:2.3,P = 0.037)是DHF的独立预测因素。在我们的研究中,总体死亡率为1.2%。
当前研究表明,DF和DHF呈现出显著不同的临床实验室特征。年龄较大、二次感染、糖尿病、嗜睡、胆囊壁增厚和延迟住院是DHF的显著预测因素。了解DHF/DSS发生的预期临床特征和预测因素,一方面可为识别高危个体提供信息,另一方面可为临床医生争取足够时间以降低登革热相关的发病率和死亡率。