Prasad Pottumarthi V, Thacker Jon, Li Lu-Ping, Haque Muhammad, Li Wei, Koenigs Heather, Zhou Ying, Sprague Stuart M
Department of Radiology, NorthShore University HealthSystem, Evanston, Illinois, United States of America.
Department of Biomedical Engineering, Northwestern University, Evanston, Illinois, United States of America.
PLoS One. 2015 Oct 2;10(10):e0139661. doi: 10.1371/journal.pone.0139661. eCollection 2015.
The current clinical classification of chronic kidney disease (CKD) is not perfect and may be overestimating both the prevalence and the risk for progressive disease. Novel markers are being sought to identify those at risk of progression. This preliminary study evaluates the feasibility of magnetic resonance imaging based markers to identify early changes in CKD.
Fifty-nine subjects (22 healthy, 7 anemics with no renal disease, 30 subjects with CKD) participated. Data using 3D volume imaging, blood oxygenation level dependent (BOLD) and Diffusion MRI was acquired. BOLD MRI acquisition was repeated after 20 mg of iv furosemide.
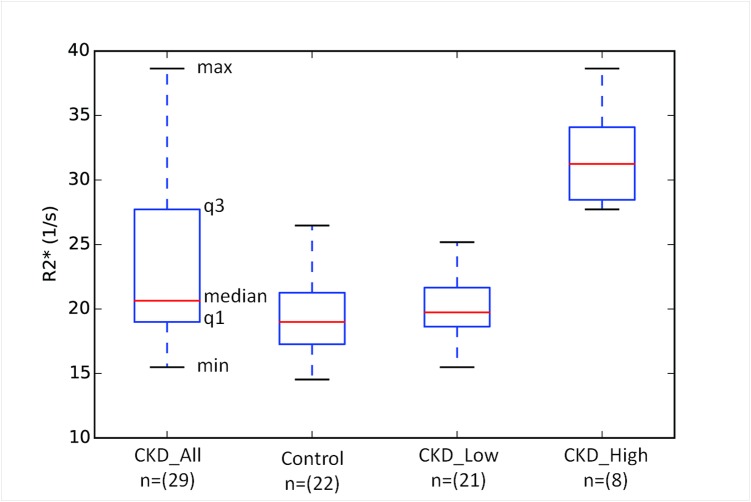
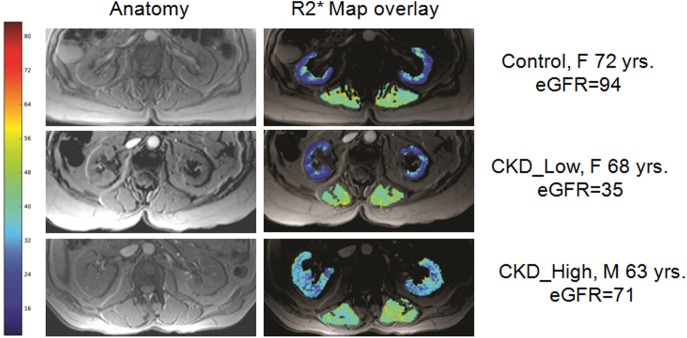
Compared to healthy subjects, those with CKD have lower renal parenchymal volumes (329.6±66.4 vs. 257.1±87.0 ml, p<0.005), higher cortical R2* values (19.7±3.2 vs. 23.2±6.3 s(-1), p = 0.013) (suggesting higher levels of hypoxia) and lower response to furosemide on medullary R2* (6.9±3.3 vs. 3.1±7.5 s(-1), p = 0.02). All three parameters showed significant correlation with estimated glomerular filtration rate (eGFR). When the groups were matched for age and sex, cortical R2* and kidney volume still showed significant differences between CKD and healthy controls. The most interesting observation is that a small number of subjects (8 of 29) contributed to the increase in mean value observed in CKD. The difference in cortical R2* between these subjects compared to the rest were highly significant and had a large effect size (Cohen's d = 3.5). While highly suggestive, future studies may be necessary to verify if such higher levels of hypoxia are indicative of progressive disease. Diffusion MRI showed no differences between CKD and healthy controls.
These data demonstrate that BOLD MRI can be used to identify enhanced hypoxia associated with CKD and the preliminary observations are consistent with the chronic hypoxia model for disease progression in CKD. Longitudinal studies are warranted to further verify these findings and assess their predictive value.
慢性肾脏病(CKD)目前的临床分类并不完善,可能高估了其患病率和疾病进展风险。正在寻找新的标志物来识别有疾病进展风险的人群。这项初步研究评估了基于磁共振成像的标志物识别CKD早期变化的可行性。
59名受试者(22名健康者、7名无肾脏疾病的贫血患者、30名CKD患者)参与研究。采集了使用三维容积成像、血氧水平依赖性功能磁共振成像(BOLD)和扩散加权磁共振成像的数据。静脉注射20mg呋塞米后重复进行BOLD磁共振成像采集。
与健康受试者相比,CKD患者肾实质体积更低(329.6±66.4 vs. 257.1±87.0ml,p<0.005),皮质R2值更高(19.7±3.2 vs. 23.2±6.3s⁻¹,p = 0.013)(提示缺氧水平更高),髓质R2对呋塞米的反应更低(6.9±3.3 vs. 3.1±7.5s⁻¹,p = 0.02)。所有这三个参数均与估计肾小球滤过率(eGFR)显著相关。当按年龄和性别匹配组时,但CKD组和健康对照组之间的皮质R2和肾脏体积仍存在显著差异。最有趣的观察结果是,少数受试者(29名中的8名)导致了CKD组观察到的平均值增加。与其余受试者相比,这些受试者的皮质R2差异非常显著,且效应量很大(科恩d值 = 3.5)。虽然极具提示性,但可能需要进一步的研究来验证这种较高的缺氧水平是否表明疾病进展。扩散加权磁共振成像显示CKD组与健康对照组之间无差异。
这些数据表明,BOLD磁共振成像可用于识别与CKD相关的缺氧增强,初步观察结果与CKD疾病进展的慢性缺氧模型一致。有必要进行纵向研究以进一步验证这些发现并评估其预测价值。