Valipour Arschang, Shah Pallav L, Gesierich Wolfgang, Eberhardt Ralf, Snell Greg, Strange Charlie, Barry Robert, Gupta Avina, Henne Erik, Bandyopadhyay Sourish, Raffy Philippe, Yin Youbing, Tschirren Juerg, Herth Felix J F
Department of Respiratory and Critical Care Medicine, Ludwig Boltzmann Institute for COPD, Otto Wagner Hospital, Vienna, Austria.
Respiration. 2015;90(5):402-11. doi: 10.1159/000439544. Epub 2015 Oct 3.
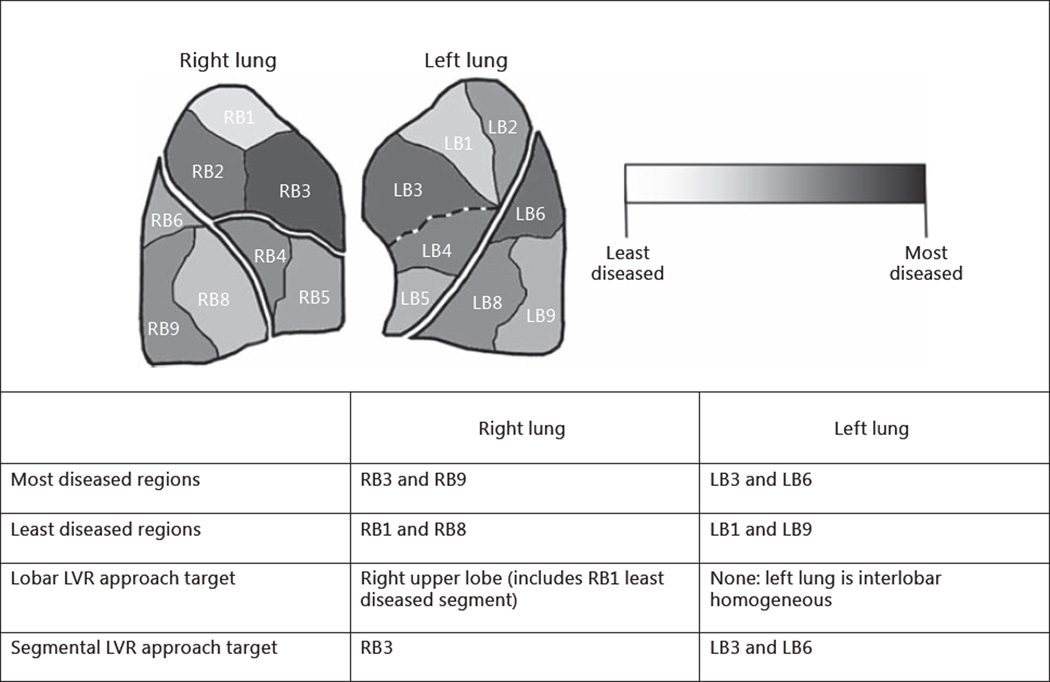
Although lobar patterns of emphysema heterogeneity are indicative of optimal target sites for lung volume reduction (LVR) strategies, the presence of segmental, or sublobar, heterogeneity is often underappreciated.
The aim of this study was to understand lobar and segmental patterns of emphysema heterogeneity, which may more precisely indicate optimal target sites for LVR procedures.
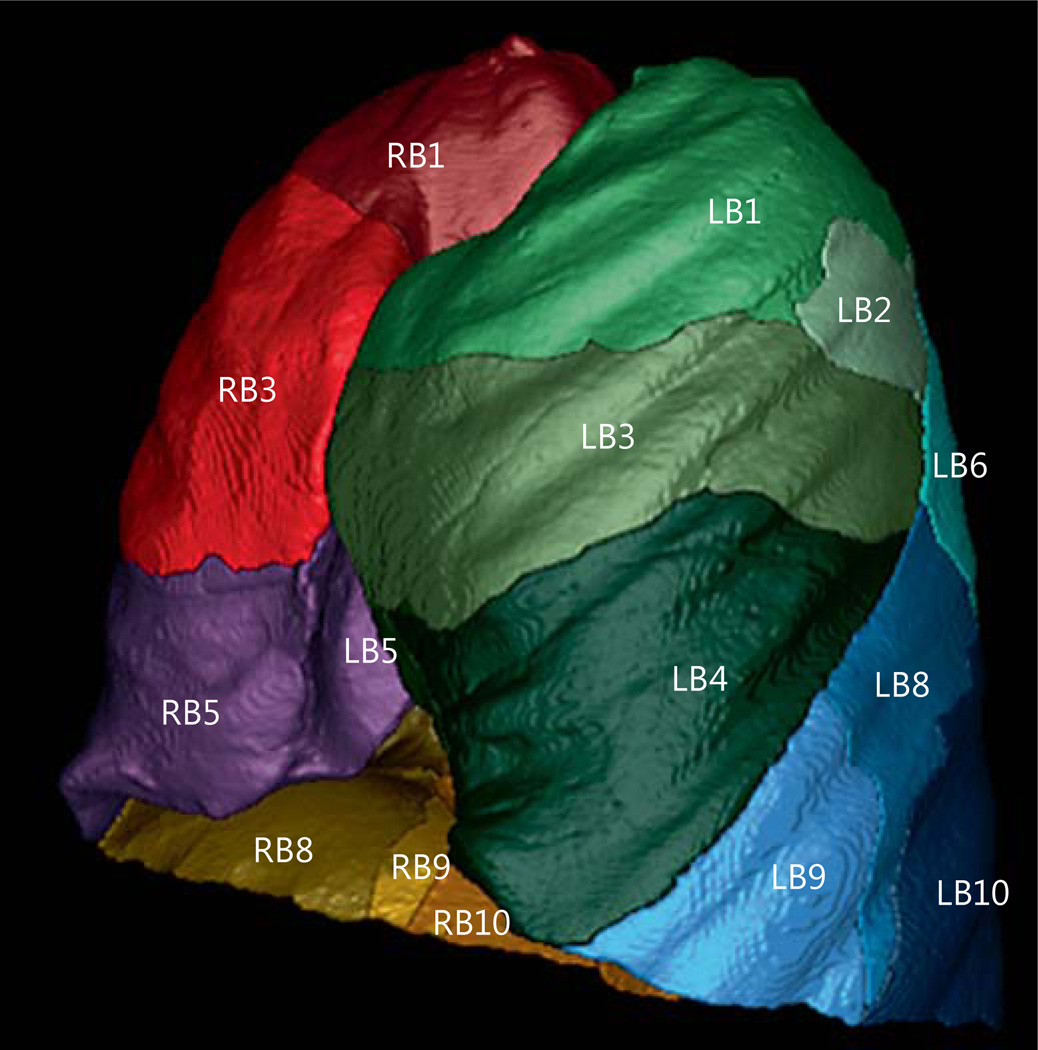
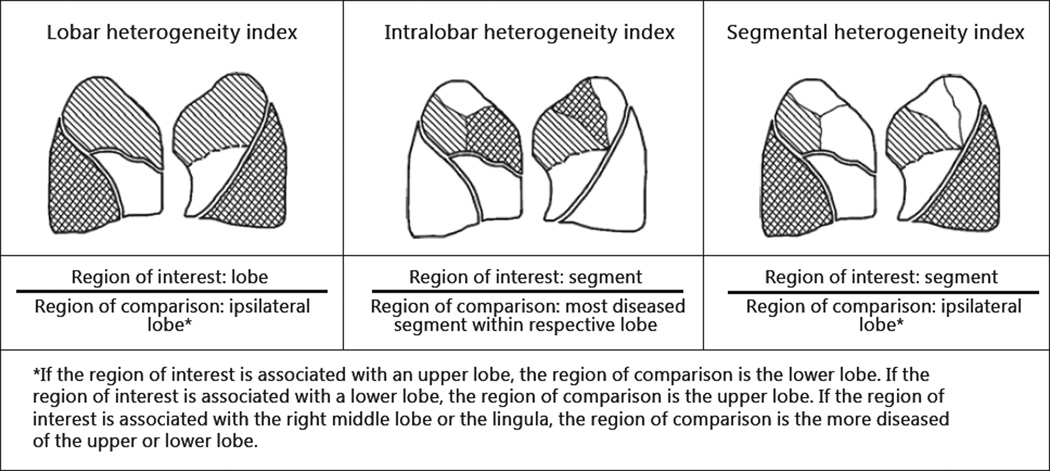
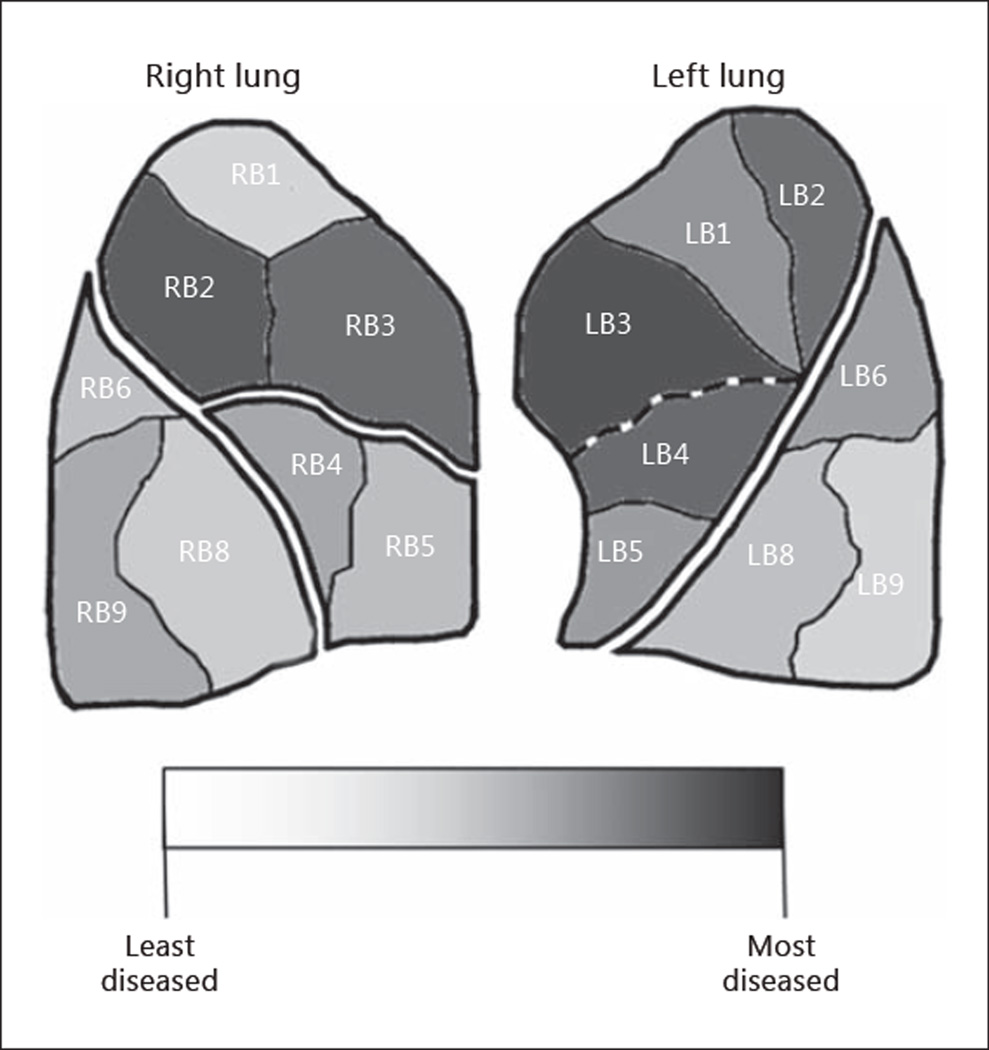
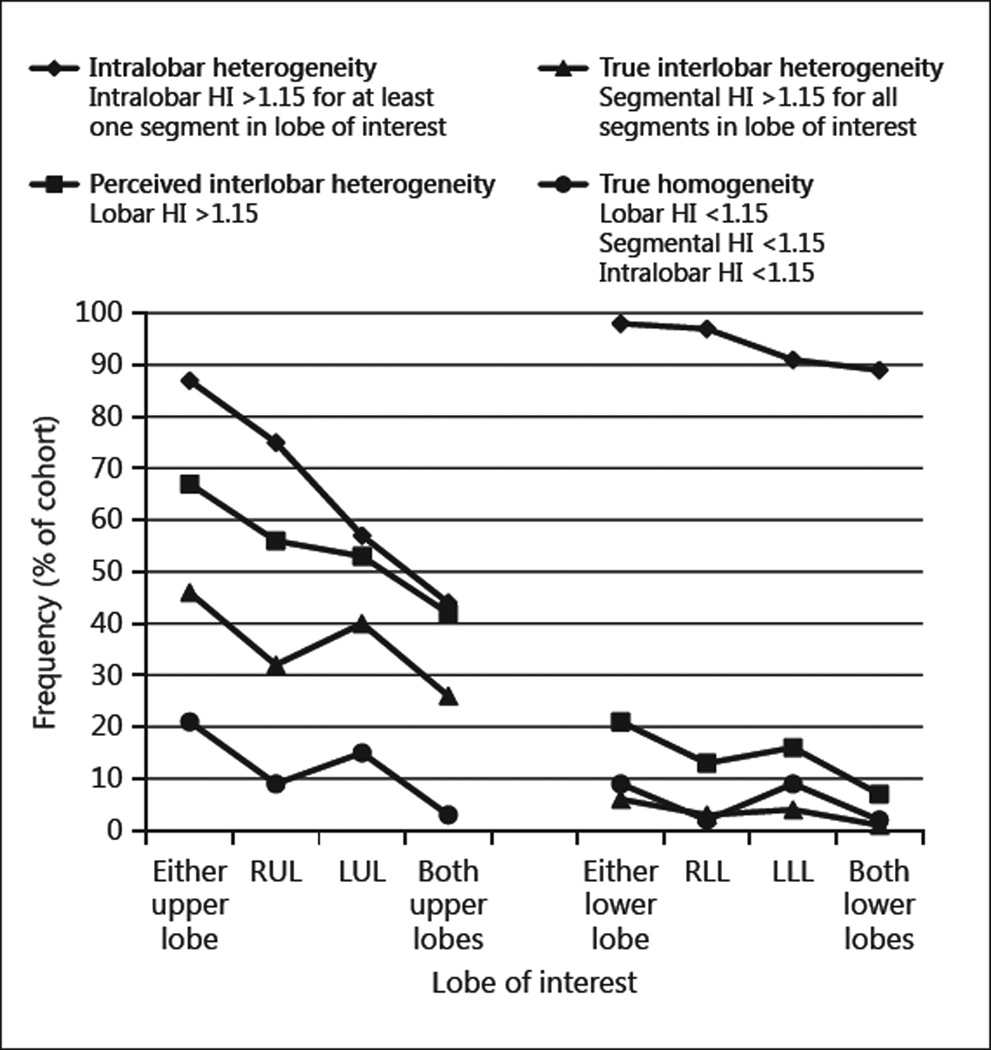
Patterns of emphysema heterogeneity were evaluated in a representative cohort of 150 severe (GOLD stage III/IV) chronic obstructive pulmonary disease (COPD) patients from the COPDGene study. High-resolution computerized tomography analysis software was used to measure tissue destruction throughout the lungs to compute heterogeneity (≥15% difference in tissue destruction) between (inter-) and within (intra-) lobes for each patient. Emphysema tissue destruction was characterized segmentally to define patterns of heterogeneity.
Segmental tissue destruction revealed interlobar heterogeneity in the left lung (57%) and right lung (52%). Intralobar heterogeneity was observed in at least one lobe of all patients. No patient presented true homogeneity at a segmental level. There was true homogeneity across both lungs in 3% of the cohort when defining heterogeneity as ≥30% difference in tissue destruction.
Many LVR technologies for treatment of emphysema have focused on interlobar heterogeneity and target an entire lobe per procedure. Our observations suggest that a high proportion of patients with emphysema are affected by interlobar as well as intralobar heterogeneity. These findings prompt the need for a segmental approach to LVR in the majority of patients to treat only the most diseased segments and preserve healthier ones.
尽管肺气肿异质性的肺叶模式表明了肺减容(LVR)策略的最佳靶位点,但节段性或亚肺叶异质性的存在常常未得到充分认识。
本研究旨在了解肺气肿异质性的肺叶和节段模式,这可能更精确地表明LVR手术的最佳靶位点。
在慢性阻塞性肺疾病(COPD)基因研究中,对150例重度(GOLD III/IV期)COPD患者的代表性队列进行肺气肿异质性模式评估。使用高分辨率计算机断层扫描分析软件测量全肺组织破坏情况,以计算每位患者肺叶间(跨叶)和肺叶内(叶内)的异质性(组织破坏差异≥15%)。对肺气肿组织破坏进行节段性特征分析以确定异质性模式。
节段性组织破坏显示左肺(57%)和右肺(52%)存在叶间异质性。所有患者的至少一个肺叶中观察到叶内异质性。在节段水平上,没有患者呈现真正的均匀性。当将异质性定义为组织破坏差异≥30%时,该队列中有3%的患者两肺均呈现真正的均匀性。
许多用于治疗肺气肿的LVR技术都集中在叶间异质性上,每次手术针对整个肺叶。我们的观察结果表明,很大一部分肺气肿患者受到叶间以及叶内异质性的影响。这些发现提示,对于大多数患者,需要采用节段性方法进行LVR,仅治疗病变最严重的节段并保留较健康的节段。