Penny Melissa A, Maire Nicolas, Bever Caitlin A, Pemberton-Ross Peter, Briët Olivier J T, Smith David L, Gething Peter W, Smith Thomas A
Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, 4051, Basel, Switzerland.
University of Basel, Petersplatz 1, Basel, Switzerland.
Malar J. 2015 Oct 5;14:384. doi: 10.1186/s12936-015-0864-3.
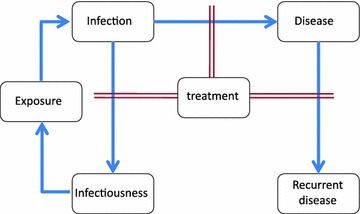
Malaria prevalence, clinical incidence, treatment, and transmission rates are dynamically interrelated. Prevalence is often considered a measure of malaria transmission, but treatment of clinical malaria reduces prevalence, and consequently also infectiousness to the mosquito vector and onward transmission. The impact of the frequency of treatment on prevalence in a population is generally not considered. This can lead to potential underestimation of malaria exposure in settings with good health systems. Furthermore, these dynamical relationships between prevalence, treatment, and transmission have not generally been taken into account in estimates of burden.
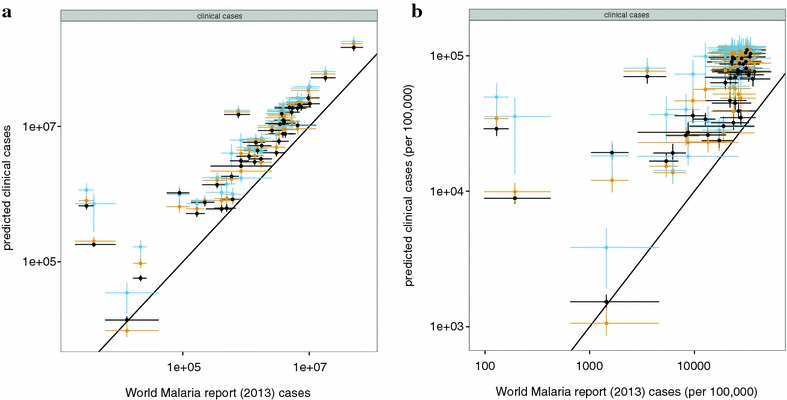
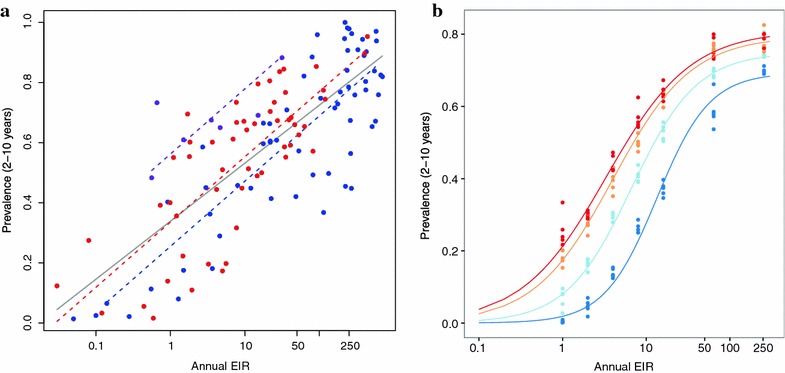
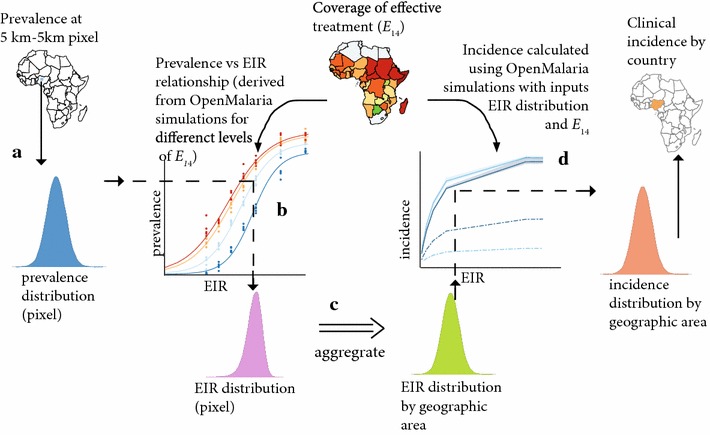
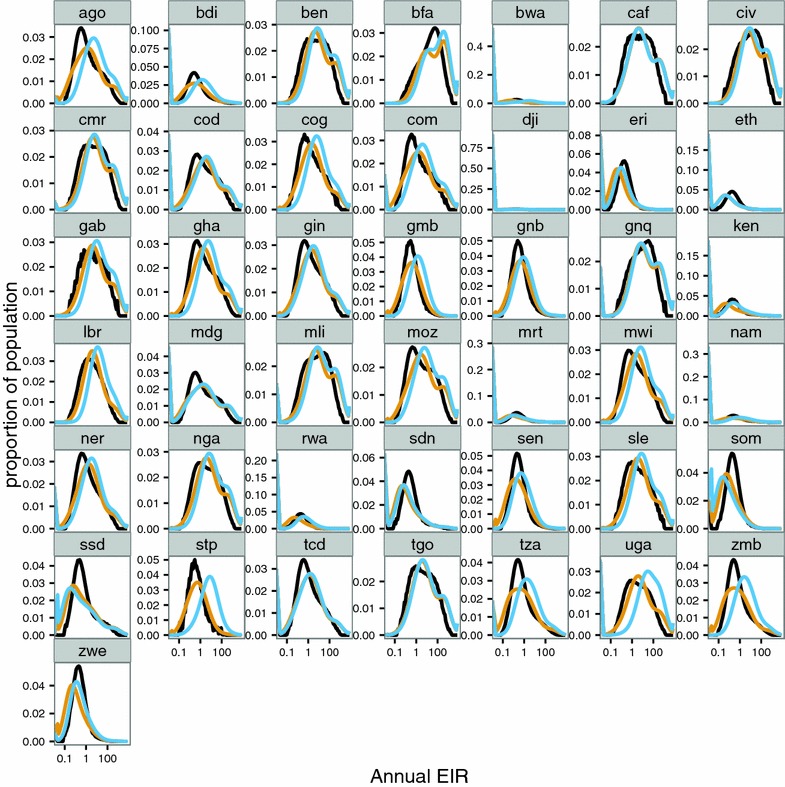
Using prevalence as an input, estimates of disease incidence and transmission [as the distribution of the entomological inoculation rate (EIR)] for Plasmodium falciparum have now been made for 43 countries in Africa using both empirical relationships (that do not allow for treatment) and OpenMalaria dynamic micro-simulation models (that explicitly include the effects of treatment). For each estimate, prevalence inputs were taken from geo-statistical models fitted for the year 2010 by the Malaria Atlas Project to all available observed prevalence data. National level estimates of the effectiveness of case management in treating clinical attacks were used as inputs to the estimation of both EIR and disease incidence by the dynamic models.
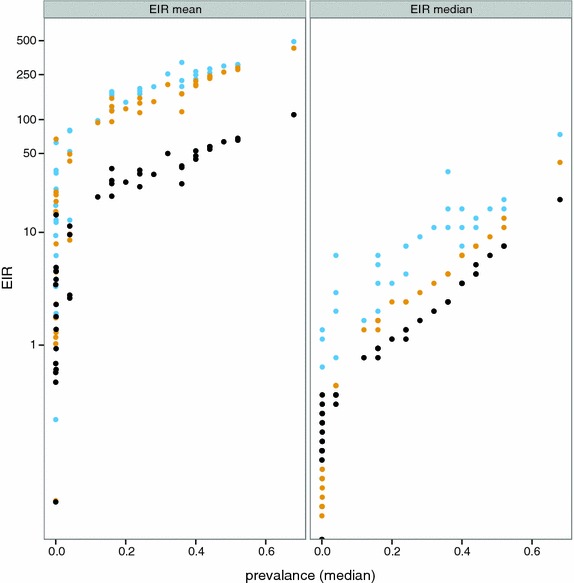
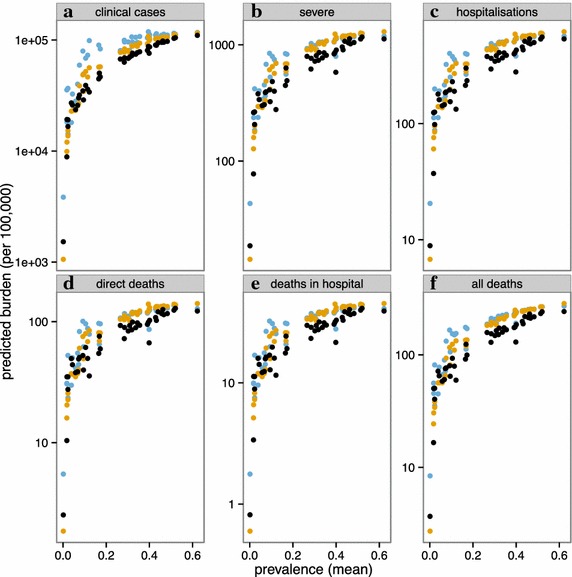
When coverage of effective treatment is taken into account, higher country level estimates of average EIR and thus higher disease burden, are obtained for a given prevalence level, especially where access to treatment is high, and prevalence relatively low. These methods provide a unified framework for comparison of both the immediate and longer-term impacts of case management and of preventive interventions.
疟疾流行率、临床发病率、治疗情况及传播率相互之间动态关联。流行率常被视作疟疾传播的一项指标,但临床疟疾的治疗会降低流行率,进而也会降低对蚊媒的传染性及后续传播。通常未考虑治疗频率对人群中流行率的影响。这可能导致在卫生系统良好的环境中对疟疾暴露情况的潜在低估。此外,在负担估计中,一般未考虑流行率、治疗及传播之间的这些动态关系。
以流行率作为输入数据,现利用经验关系(未考虑治疗因素)和OpenMalaria动态微观模拟模型(明确纳入治疗效果),对非洲43个国家的恶性疟原虫疾病发病率及传播情况(作为昆虫接种率分布)进行了估计。对于每项估计,流行率输入数据均取自疟疾地图项目为2010年拟合地理统计模型时所用的所有可获得的观察到的流行率数据。将国家层面病例管理在治疗临床发作方面的有效性估计值用作动态模型估计昆虫接种率及疾病发病率的输入数据。
考虑有效治疗的覆盖率时,对于给定的流行率水平,尤其是在治疗可及性高且流行率相对较低的情况下,会得出更高的国家层面平均昆虫接种率估计值,从而得出更高的疾病负担。这些方法为比较病例管理及预防性干预措施的近期和长期影响提供了一个统一框架。