Camponovo Flavia, Bever Caitlin A, Galactionova Katya, Smith Thomas, Penny Melissa A
Swiss Tropical and Public Health Institute, Basel, Switzerland.
University of Basel, Basel, Switzerland.
Malar J. 2017 Jan 3;16(1):1. doi: 10.1186/s12936-016-1650-6.
Appropriate treatment of life-threatening Plasmodium falciparum malaria requires in-patient care. Although the proportion of severe cases accessing in-patient care in endemic settings strongly affects overall case fatality rates and thus disease burden, this proportion is generally unknown. At present, estimates of malaria mortality are driven by prevalence or overall clinical incidence data, ignoring differences in case fatality resulting from variations in access. Consequently, the overall impact of preventive interventions on disease burden have not been validly compared with those of improvements in access to case management or its quality.
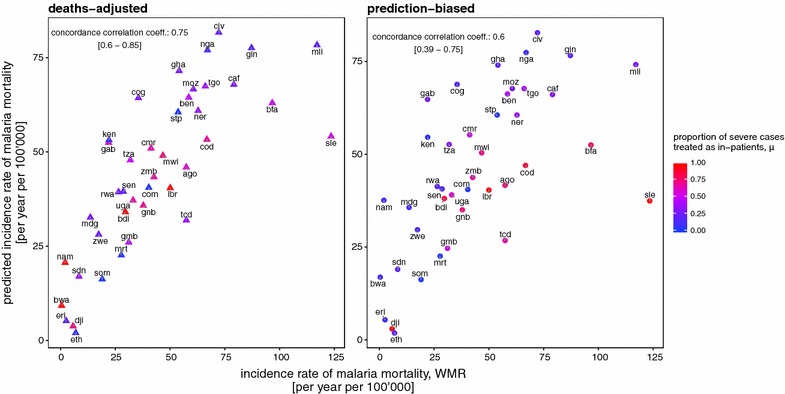
Using a simulation-based approach, severe malaria admission rates and the subsequent severe malaria disease and mortality rates for 41 malaria endemic countries of sub-Saharan Africa were estimated. Country differences in transmission and health care settings were captured by use of high spatial resolution data on demographics and falciparum malaria prevalence, as well as national level estimates of effective coverage of treatment for uncomplicated malaria. Reported and modelled estimates of cases, admissions and malaria deaths from the World Malaria Report, along with predicted burden from simulations, were combined to provide revised estimates of access to in-patient care and case fatality rates.
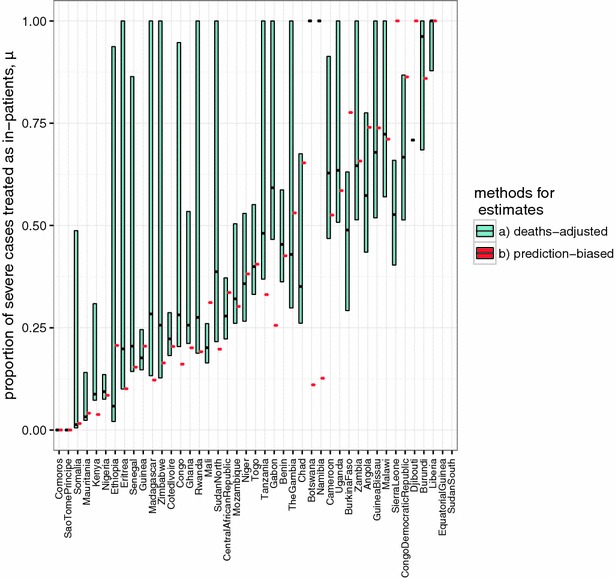
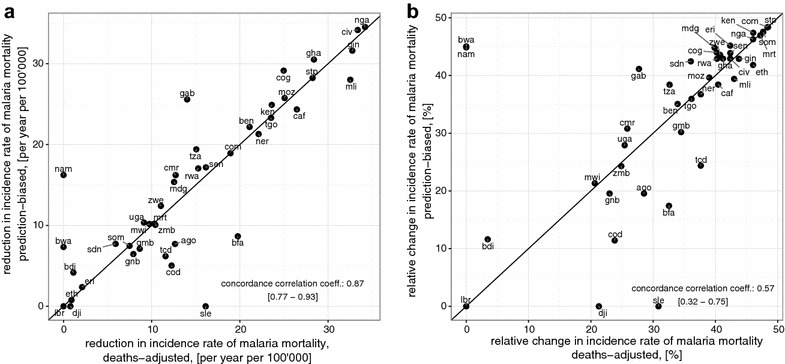
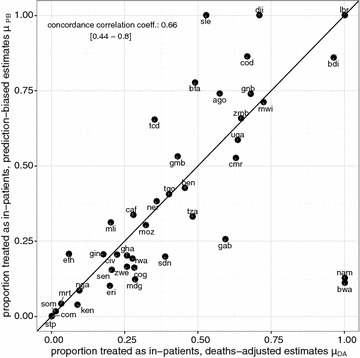
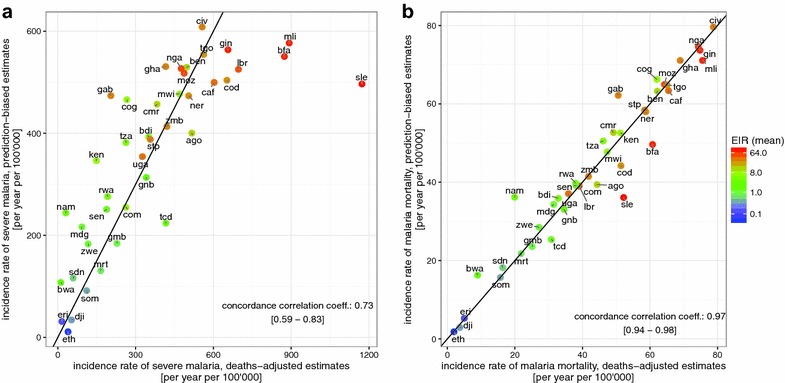
There is substantial variation between countries' in-patient admission rates and estimated levels of case fatality rates. It was found that for many African countries, most patients admitted for in-patient treatment would not meet strict criteria for severe disease and that for some countries only a small proportion of the total severe cases are admitted. Estimates are highly sensitive to the assumed community case fatality rates. Re-estimation of national level malaria mortality rates suggests that there is substantial burden attributable to inefficient in-patient access and treatment of severe disease.
The model-based methods proposed here offer a standardized approach to estimate the numbers of severe malaria cases and deaths based on national level reporting, allowing for coverage of both curative and preventive interventions. This makes possible direct comparisons of the potential benefits of scaling-up either category of interventions. The profound uncertainties around these estimates highlight the need for better data.
对危及生命的恶性疟原虫疟疾进行恰当治疗需要住院治疗。尽管在疟疾流行地区,获得住院治疗的重症病例比例对总体病死率进而对疾病负担有很大影响,但这一比例通常并不为人所知。目前,疟疾死亡率的估计是由患病率或总体临床发病率数据驱动的,忽略了因获得治疗机会不同而导致的病死率差异。因此,预防干预措施对疾病负担的总体影响尚未与改善病例管理的可及性或其质量所带来的影响进行有效比较。
采用基于模拟的方法,估计了撒哈拉以南非洲41个疟疾流行国家的重症疟疾住院率以及随后的重症疟疾疾病和死亡率。利用人口统计学和恶性疟原虫疟疾患病率的高空间分辨率数据,以及全国范围内单纯性疟疾治疗有效覆盖率的估计值,捕捉各国在传播和卫生保健环境方面的差异。将《世界疟疾报告》中报告的和模拟的病例、住院人数及疟疾死亡估计值,与模拟预测的负担相结合,以提供获得住院治疗机会和病死率的修订估计值。
各国的住院率和估计的病死率水平存在很大差异。研究发现,对于许多非洲国家来说,大多数因住院治疗而入院的患者不符合重症疾病的严格标准,而且对于一些国家来说,仅占总重症病例的一小部分被收治。估计值对假定的社区病死率高度敏感。对国家层面疟疾死亡率的重新估计表明,因住院治疗可及性不足和重症疾病治疗无效而导致的负担很大。
本文提出的基于模型的方法提供了一种标准化方法,可根据国家层面的报告估计重症疟疾病例和死亡人数,同时考虑到治疗性和预防性干预措施的覆盖情况。这使得能够直接比较扩大这两类干预措施的潜在益处。这些估计值周围存在的巨大不确定性凸显了获取更好数据的必要性。